

Special Interest Group Update
In each issue, one of NANN’s special interest groups shares information in their area of focus.
Safe Rides Home, Part II: Positioning and Harnessing Small Babies in Child Safety Seats
By Heidi Heflin, MN RN CNS CPSTI
 Learning to assist families in choosing a correctly fitted child safety seat (CSS) for premature or low-birthweight babies is complicated by the issues of their low tone, medical conditions, maturation, and size (Bull et al., 2009; reaffirmed 2018). Positioning and harnessing a small baby are, thus, more complex (Bull et al., 2009; reaffirmed 2018).
Learning to assist families in choosing a correctly fitted child safety seat (CSS) for premature or low-birthweight babies is complicated by the issues of their low tone, medical conditions, maturation, and size (Bull et al., 2009; reaffirmed 2018). Positioning and harnessing a small baby are, thus, more complex (Bull et al., 2009; reaffirmed 2018).
Federal Motor Vehicle Safety Standard (FMVSS) 213 requirements of CSSs do not meet the specific positioning and transportation needs of these small babies because it is difficult to simulate low tone and airway fragility in a crash test dummy (O’Neil et al., 2019., Bull et al., 2009; reaffirmed 2018). Although CSS manufacturers have created options for smaller babies, the seats generally have complicated multistep instructions and extra parts, increasing the risk of misuse. This makes the job of the neonatal nurse who educates families or performs the car seat tolerance screening (CSTS) that much more difficult.
Proper selection and use of CSSs are important for ensuring that all children are transported as safely as possible. Guidance for selection of CSS for smaller babies can be found in the January issue of NANN E-Newsin “Safe Rides Home for Smaller Babies” (Heflin & Siemion, 2021).
Just as important as proper selection and use are correct positioning and harnessing. Infants that tolerate a semi-reclined position should ride in a conventional (a rear-facing-only or convertible) CSS, facing the rear of the vehicle, properly positioned, and in a snug five-point harness (Bull et al., 2009; reaffirmed 2018). A correctly used harness secures the rear-facing child during a frontal collision by keeping the body low in the seat. The head and neck move together with the CSS, allowing the crash force to be spread across the CSS shell, thus decreasing the risk for neck and/or spine injury (National Highway Traffic Safety Administration et al., 2020).
However, smaller babies often fit poorly in standard CSSs. The harness may not fit snugly, and the straps and buckles may fall in the wrong places (Davis et al., 2020). Neonates can slump easily in an ill-fitted seat. The infant’s head flops forward, occluding the airway, and newborns do not have the strength for repositioning (Davis et al., 2020). Although this creates a challenge, following specific steps for proper positioning and correct harness use reduce risk.
It is essential to follow the manufacturer’s instructions (MI) for each specific CSS, to learn how to position baby in the seat in which they will be traveling home (Bull et al., 2009; reaffirmed 2018), to understand the use of manufacturer-approved features (harness threading and padding) that improve or interfere with small-baby fit, and to learn how to test for harness snugness. Nurses who conduct the CSTS need to be trained in positioning infants properly in CSSs (Bull et al., 2009; reaffirmed 2018), including the requirement to read and follow manufacturers’ instructions. These skills are best taught to nurses through hands-on training and then reviewed during annual competencies by the CPS expert, the Child Passenger Safety Technician (CPST), a nationally certified educator in the field of occupant protection. When possible, defer safe transportation questions for children with special healthcare needs to a CPST with Special Needs training and appropriately trained for children with medical conditions that involve special positioning requirements or considerations for travel (American Academy of Pediatrics et al., 2014).
Manufacturer’s instructions direct the user toward the adjustments that are necessary for proper use. To learn which unique features the CSS has to fit the small baby, nurses must consult the MI every time they use a CSS. Each one of the 400+ different CSSs (J. J. Stubbs, personal communication, March 15, 2021) in use in the U.S. has unique instructions specific to models, years, modes in which the seat is used, child’s size, and the direction of the seat during transport. Using the MI is the only way to ensure the use of the CSS in its crash-tested mode. Unfortunately, MI are not always easily accessible and, by design, are very detailed and lengthy. To track down the MI of a specific CSS, go to that manufacturer’s website. Directions frequently can be found under the heading ‘Support’. For specific directions on positioning and harnessing, look at ‘Securing the Child’ or ‘Harness or Buckle Adjustment’ within the MI. To help professionals, like themselves, working with a variety of CSSs, the non-profit organization SafetyBeltSafe U.S.A. created an online resource (found on www.carseat.org). The Child Restraint Manufacturers’ Instructions with Summaries is a compilation of manufacturers’ instructions for all CSSs made in the past 10 years. In addition, each MIs comes with a summary containing revised recommendations from manufacturers, harness threading, identification images, and more. These one-to-three-page summaries highlight manufacturer’s steps to follow for correct CSS use but in a shortened format. The summaries are not a substitute for the MI but a guide to them.
Frequently, the CSS must be adjusted before use for smaller babies, especially if it is an older sibling’s hand-me-down. There are a few new seats that arrive out of the box set up for larger babies as well and need to be changed so the straps fit snugly to the child’s body. Adjustment of a harness depends on the type of harness (rethread vs. no-rethread) found on the CSS. The name describes its mechanism of adjustment. A ‘rethread harness’ requires the harness to be detached and rethreaded in and out of the CSS plastic shell into different slots. A ‘rethread harness’ has shoulder harness slot choices to adjust the position relative to the infant’s shoulder height and/or hip width. Adjustments should be done prior to buckling baby in (National Highway Traffic Safety Administration et al., 2020). A ‘no-rethread harness’ allows for shoulder height adjustment with a lever or button to move the height up or down, usually by raising or lowering the headrest. This type of harness never is unthreaded from the shell. When using a CSS rear facing, the harness is placed on the shoulders and adjusted to enter the shell at slots in line with or below the child’s shoulders (National Highway Traffic Safety Administration et al., 2020). A few seats have multiple hip (waist) harness slots and/or multiple buckle (crotch) strap locations. Shortening the buckle strap is sometimes available, too. In addition, some rethread harnesses come with an option to shorten the harness webbing by providing optional smaller-baby loops to attach to the metal splitter plate found on the back of the seat. Learning to read, understand, and follow the MI is painstaking. Therefore, it is recommended nurses receive education and support from a CPST (American Academy of Pediatrics et al., 2014). Although not a substitute for the support of a CPST on the hospital team, many manufacturers offer virtual help through their websites.
Some conventional CSSs have features (either required or optional) to assist in positioning; refer to CSS manufacturer’s instructions and national guidance from the AAP for positioning preterm and low-birth-weight infants (Bull et al., 2009; reaffirmed 2018). A properly positioned child has the buttocks and back flat against the back of the CSS. A manufacturer’s approved padding and inserts (head pillow, body pillow, harness covers, and buckle pads) can boost the baby to provide a better harness fit and/or provide lateral support against slumping.
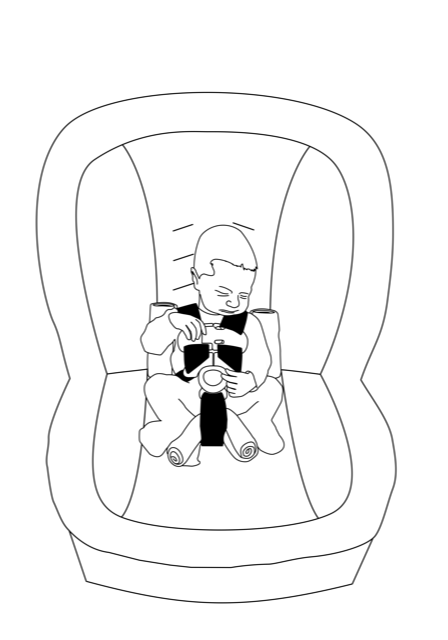
Not all new seats come with these additional parts, and reused seats may have parts missing (check the MI). When reusing a CSS, all parts MUST be accounted for. If these extra parts do not come with a new seat, it does not necessarily preclude choosing the seat for a small baby. It may be possible to place rolled receiving blankets along both sides of the body to shoulder level (avoiding the face and head) to prevent slumping and/or a small, rolled washcloth between the baby and the buckle (crotch) strap to prevent submarining (Bull et al., 2009; reaffirmed 2018) (see illustration). Warning! Blankets or padding placed behind the baby or under the harness will interfere with the effectiveness of the harness, putting the baby at risk of ejection in a sudden stop or crash (National Highway Traffic Safety Administration et al., 2020). There may be instances when the approved padding or inserts interfere with a good fit and when designated ‘optional’ by the manufacturer, they may be removed. For example, the head pillow of some seats may push the smaller neonate’s head forward, risking occlusion of the airway and, when designated ‘optional,’ may be removed. All padding, blankets, or insert add-ons to the CSS must be approved by the manufacturer in the instructions, on the manufacturer’s official website, or through verbal approval from the CSS manufacturer. Adding unapproved extras to a CSS can compromise the integrity, void the warranty, and impact safety and overall performance. To learn how and when to use inserts and padding, ask a CPST to demonstrate use of these CSS parts or ask the manufacturer to offer an in-service on the use of their CSS.
Once the harness is adjusted and baby is positioned and buckled in, the harness must be tightened to a snug fit. Pull the strap taut from the hips through the buckle and up the front of the chest, ensuring no webbing is left loose. Most harnesses can be tightened by pulling the harness adjuster strap. A snug harness is judged by ensuring that the harness webbing cannot be pinched between thumb and forefinger. Once snugged, as the final step, the chest clip is fastened and then pushed to the midpoint of the infant’s chest at armpit level.
New options in CSS help small babies fit in seats originally made for larger babies. While a variety of adjustable components may enhance the performance of a CSS for a small baby, making the necessary adjustments can be complicated and somewhat overwhelming, and misuse may be even more prevalent for this population. Hoffman et al. (2014) found that families that worked with a CPST were significantly less likely to misuse their CSS; the same presumption can be applied to the neonatal nurse. Utilizing a CPST as a resource for the neonatal team can help keep staff trained and updated and assist with problem-solving in complex CSS cases. To support nurses responsible for harnessing neonates for the CSTS and educating parents in proper CSS use, there should be hands-on training from a CPST to protect a nurse’s practice, patients, and institution. Early involvement of a CPST for staff and caregiver education may decrease the number of infants who have unstable cardiorespiratory status in the CSS due to improper positioning or poor fit (Davis & Cheo, 2021) thus, potentially decreasing readmission, poor outcomes, failed CSTS, and possible delays in hospital discharge.
This article is not a substitute for hands-on training! Additional resources and where to find a CPST can be found in the January issue of NANN E-News entitled Safe Rides Home for Smaller Babies (Heflin & Siemion, 2021).
Our Sponsor
