

Special Interest Group Update
In each issue, one of NANN’s special interest groups shares information in their area of focus.
Complexities of BPD: It's Not Just the Alveoli
Understanding phenotypes and the challenges of Bronchopulmonary Dysplasia definitions
Jennifer L. Wilson, MS CRNP NNP-BC
As neonatal nurses, our primary diagnosis treated in the NICU is respiratory distress or respiratory distress syndrome (Harrison & Goodman, 2015). Infants can have respiratory distress from many types of etiology, including retained fetal lung fluid, pulmonary hypertension, pneumonia, surfactant impairment or surfactant deficiency. When the primary etiology is surfactant deficiency or impairment, the diagnosis is then respiratory distress syndrome or RDS (Wilson & Fitzgerald, 2019). If the infant continues to have respiratory distress and an oxygen requirement, at what point do we define the lung disease as bronchopulmonary dysplasia (BPD), and what role do the components of alveolar disease, obstructive disease, and vasculature disease play in long-term outcome?
To better understand and define these other factors, knowledge of the respiratory phenotypes is essential for the neonatal nurse. Consensus on the definition of BPD has been difficult, with current definitions lacking radiological, laboratory, and histopathologic findings.
Background
Premature infants often miss the last stage of alveoli growth and proliferation. The canicular phase of lung development occurs between 19 and 26 weeks of age. During this phase, continued growth of bronchioles occurs with increased proliferation of the pulmonary vasculature. At 20–22 weeks gestation, surfactant production begins but remains minimal. Type II pneumocytes, which are responsible for surfactant production, are not established until closer to the saccular phase of lung development (Moore, Persaud, & Torchia, 2020).
If an infant is born during the canicular phase, the integrity and structure of the young alveoli is fragile. With limited surfactant production, it is difficult for the alveoli to maintain the surface tension needed for gas exchange to occur. Hypoxia and hypercarbia, in the extremely premature infant is oftentimes due to lack of alveoli and the supporting vascular structure.
Signs of respiratory distress syndrome are due to this lack of effective surfactant. Surfactant deficiency or inactivation from a caustic exposure of infection, inflammation, or particulate from meconium causes presentation of the signs we see in respiratory distress: nasal flaring, retractions, grunting, and tachypnea. Each of these signs are compensatory mechanisms: nasal flaring is an effort to reduce airway resistance, grunting is an effort to prevent alveolar collapse, intercostal and subcostal retractions are auxiliary muscle use, and tachypnea is an effort to improve tidal volume (Wilson & Fitzgerald, 2019).
Surfactant replacement therapy aids in decreasing surface tension and improving gas exchange (Wilson & Fitzgerald, 2019). In addition to surfactant replacement therapy, the treatment used for RDS includes mechanical ventilation and oxygen therapy. Both treatments place risk to damage the alveoli and vasculature structures and risk the development of BPD (Keller & Ballard, 2019).
The definition and contributing etiologies of BPD remain a challenge. Why some infants go on to develop BPD and others do not is still unknown. Several factors, including genetics; infection and/or inflammation (both in-utero and during the NICU hospitalization course); oxidant injury from reactive oxygen species; and mechanical ventilation strategies, have all been linked to an increased likelihood of developing BPD. Prematurity remains the highest indicator in developing RDS and BPD, with gestational age inversely related; the younger the infant, the higher risk of developing RDS and subsequently BPD. Infants are at risk for developing BPD with any iatrogenic or inflammatory process that impairs the growth or disrupts the integrity of the alveoli and adjacent vasculature (Collaco & McGrath-Morrow, 2018).
History of BPD definitions
Bronchopulmonary dysplasia is primarily a disease of prematurity, first described over 50 years ago by Dr. William Northway and colleagues (Northway, Rosan, & Porter, 1967). They diagnosed the disease based on findings at the time of autopsy with noted changes in the alveoli, airway musculature, pulmonary arterioles and presence of right ventricular hypertrophy. This term was first used to illustrate the pathological findings that Dr. Northway and colleagues noted of premature infants who died of respiratory failure. Dysplasia was seen as the finding in patients to have died from BPD, so the presence of dysplasia became the defining feature of the disease.
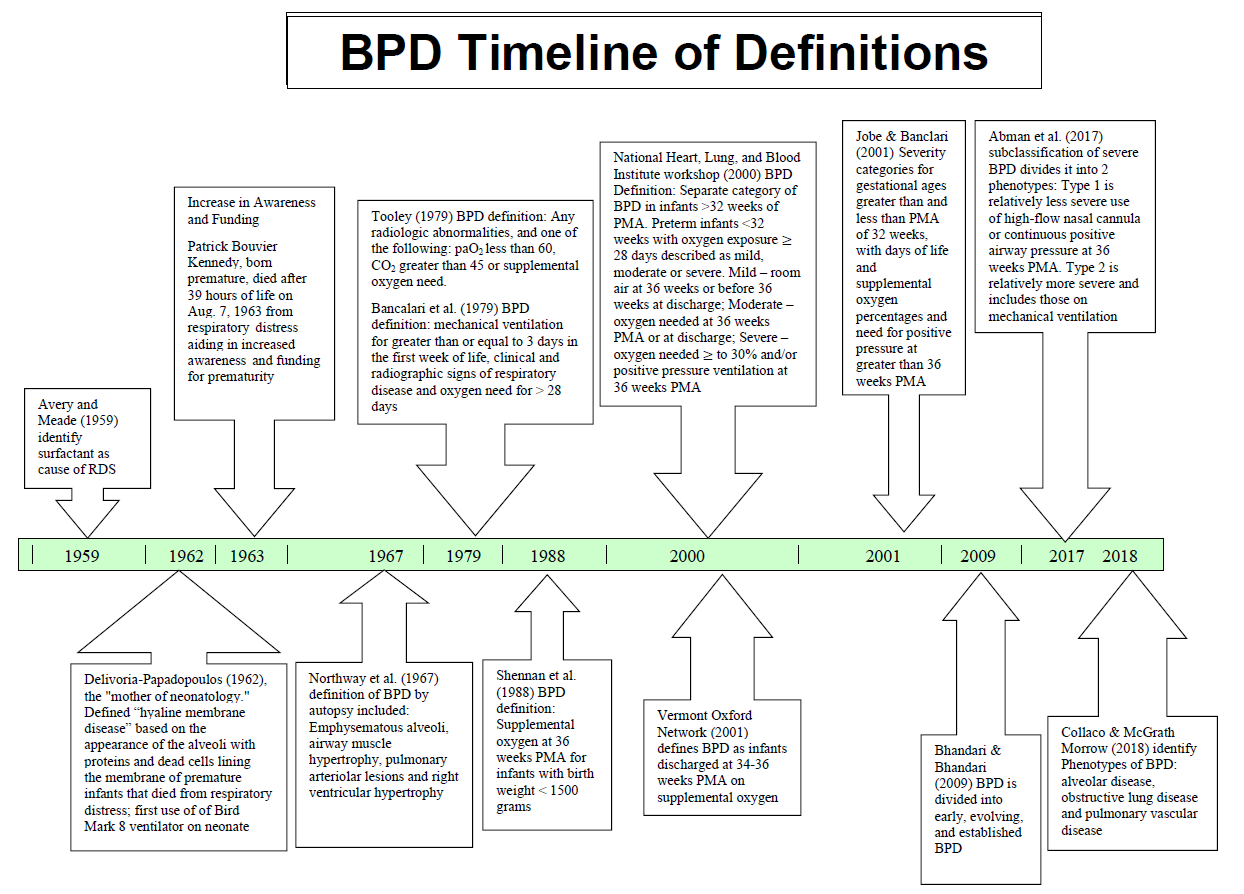
Over time, bronchopulmonary dysplasia has been defined in many ways, with the challenge of identifying it based on the pathology of the diseased lung or the treatment needed. Although there is not yet consensus regarding radiographic imaging, it has been used historically to aid in diagnosis. Subsequent definitions have included oxygen needed, oxygen levels and carbon dioxide levels. Definitions used in research have varied based on treatment needed with the assumption that the degree of diseased lung is worse in those that need increased respiratory support (Shennan, Dunn, Ohlsson, Lennox, & Hoskins, 1988; Horbar, Rogowski, Plsek, Delmore, Edwards, Hocker, et al., 2001; Bhandari & Bhandari, 2009; Jobe & Steinhorn, 2017; Day & Ryan, 2017; Collaco & McGrath-Morrow, 2018).
The timeline below highlights changes in descriptors and definitions for BPD.
Recognition of phenotypes of BPD
With improvements in ventilation strategies and standard of care to include surfactant therapy in the late 1980s, a new type of BPD has been identified. The defining characteristics include alveolar hypoplasia, remodeling of vascularity to be more simplified or poorly developed, and a delay in the normal development of lung growth (Collaco & McGrath-Morrow, 2018; Day & Ryan, 2017).
BPD is the most common disease of prematurity (Harrison & Goodman, 2015), and after asthma, it is the most common chronic pediatric respiratory disease (Collaco & McGrath-Morrow, 2018). Bronchopulmonary dysplasia is only one presenting diagnosis, and many patients have multiple phenotypes that contribute to respiratory illness. Collaco and McGrath-Morrow (2018) describe a new definition of BPD with consideration of the alveolar, obstructive, and vascular phenotypes implicated in respiratory illnesses.
Alveolar disease and the injury that occurs with use of positive pressure ventilation contributes to BPD. As PMA advances, if the need for use of positive pressure and supplemental oxygen occurs, the infant's condition is defined as BPD based on the 2001 National Heart, Lung, and Blood Institute (NHLBI) BPD definition. Therapies to improve alveolar proliferation and integrity are focused on avoiding infection, decreasing inflammation, and avoiding exposure of mechanical ventilation and environmental toxins. Monitoring of growth and providing optimal nutrition also aids in overall support of growth and recovery from iatrogenic mechanical ventilation injury (Keller & Ballard, 2019).
Obstructive processes also play a role although these processes are not part of the definition of BPD. Obstruction often presents with asthma-like symptoms due to the inflammation present in the airways. While the obstructive lung disease phenotype is not considered in the definition of BPD, obstruction has been found to possibly have lifetime implications of higher risk of virus infections requiring hospitalization (Miller et al., 2012) and continue asthma-like symptoms with need for long-term inhaled corticosteroid use.
Pulmonary vascular disease refers to mechanisms that contribute to BPD based on the relationship between the alveoli and the pulmonary vascular bed. Worsening BPD can be a result of pressures within the vasculature as well as the presence, perfusion, and number of vessels to support the pulmonary vascular bed. Pulmonary hypertension, or increased pressures within the pulmonary arteries, can lead to right ventricular hypertrophy and eventual heart failure due to BPD. Development of the necessary pulmonary vascular bed is needed to support the alveoli, and research indicates that the relatively hyperoxic environment (compared to in-utero) has a negative influence on the growth of lung vasculature (Thomas et al., 2011). The alveoli facilitate gas exchange based on the amount of surface tension and functional residual capacity, but the vasculature surrounding the alveoli must be developed and well perfused to carry the needed oxygen throughout the body and eliminate carbon dioxide.
Further research and understanding outcomes
Using this new definition, outcomes can be focused on the phenotype exhibited. Each of these phenotypes—alveolar, obstructive, and vascular—should be considered in the patient with BPD. Infants with an oxygen requirement and with the primary BPD phenotype of alveolar disease have an increase in alveolarization over the first year of life, which can optimistically improve lung function and increase the likelihood of weaning from respiratory support. In contrast, obstructive lung disease, which presents with asthma-like symptoms, is less likely to resolve during childhood. Structural changes in the airway and inflammatory processes that lead to obstruction can cause lifelong asthma symptoms. The vascular phenotype accounts for a large component of persistent BPD, often going unrecognized. Pulmonary hypertension can be difficult to capture diagnostically, and biomarkers for following pulmonary hypertension across the lifespan are still being researched (Collaco & McGrath-Morrow, 2018). Subclinical ventricular dysfunction has been found in school-age children with a history of pulmonary hypertension (Kwon et al., 2016). Because pathology is different, risk of long-term sequelae and recovery from BPD also varies.
It is important to understand and recognize the phenotypes of BPD as well as the complexity of alveolar, obstructive, and pulmonary vasculature processes, which should be studied separately to understand outcomes. In particular, understanding relationships may help to assess the infant's readiness to begin oral feeding. Respiratory fragility in severe BPD often will cause delays in introduction of and complications with oral feedings. Infants needing multi-disciplinary approaches and referral to a clinic specializing in feeding issues in patients with a comorbidity of BPD should be considered (Abman et al., 2017). These aerodigestive clinics have been created in many academic and large hospital systems with the goal of developing a multi-disciplinary approach to diagnosing and treating patients with complex pulmonary and feeding/swallowing problems (Boesch et al., 2018). The aerodigestive specialty is an emerging science, and research is needed to understand the long-term effects of the comorbidity of feeding and BPD.
Further outcomes research should focus on morbidity and mortality associated with alveolar, obstructive, or pulmonary vascular disease processes. Pulmonary outcomes are different based on the phenotype of BPD, so recognition of these pathologies is essential for quality outcomes research. Current definitions focus on the treatment that is needed at particular PMAs, rather than the actual disease process. In recognizing the phenotypes and associated pathology, the nurse can better understand the pathology of respiratory illness of BPD.
References:
- Abman, S. H., Collaco, J. M., Shepherd, E. G., Keszler, M., Cuevas-Guaman, M., Welty, S. E., Truog, W. E., McGrath-Morrow, S. A., Moore, P. E., Rhein, L. M., Kirpalani, H., Zhang, H., Gratney, L. L., Lynch, S. K., Curtiss, J., Stonestreet, B. S., McKinney, R. L., Dysart, K. C., Gien, J., Baker, C. D., et al. (2017). Interdisclipinary care of children with severe bronchopulmonary dysplasia. Journal of Pediatrics, 181(2), pp. 12-28. doi:10.1016/j.jpeds.2016.10.082.
- Avery, M. E. & Mead, J. (1959). Surface properties in relation to atelectasis and hyaline membrane disease. AMA American Journal of Disesase of Childhood, 97(5), pp 517-523. doi:10.1001/archpedi.1959.02070010519001
- Bancalari, E., Abdenour, G. E., Feller, R., Gannon, J. (1979). Bronchopulmonary dysplasia: Clinical presentation. Journal of Pediatrics, 11(95) 819-823. doi:10.1016/s0022-3476(79)080442-4.
- Bhandari, A. & Bhandari, V. (2009). Pitfalls, problems, and progress in bronchopulmonary dysplasia. Pediatrics, 123(6), pp. 1562-1573. doi:10.1542/peds.2008-1962.
- Boesch, R. P., Balakrishnan, K., Acra, S., Benscoter, D. T., Cofer, A., Collaco, J. M., Dahl, J. P., Daines, C. L., DeAlarcon, A., DeBoer, E. M., Deterding, R. R., Frielander, J. A., Gold, B. D., Grothe, R. M., Hart, C. K., Kazachkov, M., Lefton-Greif, M. A., Miller, C. K., Moore, P. E., Pentiuk, S. et al. (2018). Structure and functions of pediatric aerodigestive programs: A concensus statement. Pediatrics, 141(3). doi:10.1542/peds.2017-1701.
- Collaco, J. M. & McGrath-Morrow, S. A. (2018). Respiratory phenotypes for preterm infants, children and adults: Bronchopulmonary dysplasia and more. Annals of the American Thoracic Society, 15(5) 530-538.
- Collaco, J. M. & Abman, S. H. (2018). Evolving challenges in pediatric pulmonary medicine: New opportunities to reinvigorate the field. American Journal of Respiratory and Critical Care Medicine, 198(6), 724-729. doi:10.1164/rccm.201709-1902PP
- Day, C. & Ryan, R. (2017). Bronchopulmonary dysplasia: new becomes old again! Pediatric Research, (81) 210-213. doi:10.1038/pr.2016.201
- Delivoria-Papadopoulos, M. & Swyer, P. R. (1964). Assisted ventilation in terminal hyaline membrane disease. Archives of Disease in Childhood, 39(207), pp.481-484. doi:10.1136/adc.39.207.481.
- Harrison, W. & Goodman, D. (2015). Epidemologic Trends in neonatal intensive care, 2007-2012. Journal of the American Medical Association Pediatrics, 169(9), 855-862. doi:10.1001/jamapediatrics.2015.1305
- Higgins, R. D., Jobe, A. H., Koso-Thomas, M. Bancalari, E., Viscardi, R. M., Hartert, T. V., Ryan, R. M., Kallapur, S. G., Steinhorn, R. H., Konduri, G. G., Davis, S. D. Theabaud, B, Clyman, R. I., Collaco, J. M., Martin, C. R., Woods, J. C. Finer, N. N. & Raju, T. N. (2018). Bronchopulmonary dysplasia: Exective summary of a workshop. Journal of Pediatrics, 6(197), 300-308. doi:10.1016/j.jpeds.2018.01.043.
- Horbar, J. D., Rogowski, P. E., Plsek, P. E., Delmore, P., Edwards, W. H., Hocker, J. Kantak, A. D., Lewallen, P., Lewis, W., Lewit, E. McCaroll, C. J., Mujsce, D. Payne, N. R., Shiono, P., Soll, R. F., Leahy, K. & Carpenter, J. H. (2001). Collobarative quality improvement for neonatal intensive care. NIC/Q project investigators of the Vermont Oxford Network. Pediatrics, 107(1) 14-22. doi:10.1542/peds107.1.14
- Jobe A. H. & Bancalari, E. (2001). Bronchopulmonary dysplasia. American Journal of Respiratory and Critical Care Medicine, 163(7), pp. 1723-1729. doi:10.1164/ajrccm.163.7.2011060
- Jobe, A. H. & Steinhorn, R. (2017). Can we define bronchopulmonary dysplasia? The Journal of Pediatrics, 188(9), 19-23. doi:10.1016/j.jpeds.2017.06.064
- Keller, R. L. & Ballard, R. A. (2019). Bronchopulmonary Dysplasia. In C. Gleason & S. Juul (Eds.) Avery's Diseases of the Newborn. Philadelphia, PA: Elsevier Publishing Co.
- Moore, K. L., Persaud, T. V. N. & Torchia, M. G. (2020). Before We Are Born: Essentials of Embryology and Birth Defects. Philadelphia, PA: Elsevier Publishing Co.
- Miller, E. K., Bugna, J., Libster, R., Shepherd, B. E., Scalzo, P. M., Acosta, P. L., Hijano, D., Reynosi, N., Batalle, J. P., Coviello, S., Klein, M. I., Bauer, G., Benitez, A., Kleeberger, S. R., & Polack, F. P. (2012). Human rhinoviruses in severe respiratory disease in very low birth weight infants. Pediatrics, 129(1) e60-e67. doi:10.1543/peds.2011.0583.
- Northway, W. H., Rosan, R.C. & Porter, D. Y. (1967). Pulmonary disease following respiratory therapy of hyaline-membrane disease-bronchopulmonary dysplasia. New England Journal of Medicine, 276 357-368.
- Shennan, A. T., Dunn, M. S., Ohlsson, A., Lennox, K. & Hoskins, E. M. (1988). Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period. Pediatrics. 82, 527–32.
- Tooley, W. H. (1979). Epidemiology of bronchopulmonary dysplasia. The Journal of Pediatrics, 5(95), 851-855. doi: 10.1016/S0022-3476(79)80451-5
- Wilson, J. L. & Fitzgerald, J. (2019). The respiratory system. Fetal and Neonatology for the Advanced Practice Nurse. New York: Springer Publishing Co.
Our Sponsor
