

From the Hill to the NICU
Bi-Monthly Advocacy Updates
NANN's Health Policy and Advocacy Committee (HPAC) is committed to advocating for optimized care, and health outcomes for neonates and their families. In an effort to raise awareness of key regulations and issues that affect NANN, NANN-AP, and the populations we serve, the HPAC Committee will be sending out bi-monthly updates to help keep you informed.
March 2024 - Provision of Human Milk: The Importance of Awareness and Advocacy
By: Lisa Davenport, DNP, RN, RNC-NIC
Breastmilk has multiple health benefits for babies by providing perfect nutrition for neonatal growth and development and protecting babies from illness by providing much-needed antibodies. Babies who receive breastmilk have a decreased incidence of asthma, type I diabetes, sudden infant death syndrome, decreased infections, and stomach viruses (CDC, 2023), and premature babies who receive breastmilk receive even more benefits such as better digestive, brain, and eye development (Nationwide Children’s, 2022). Despite numerous medical advances in recent years, the preterm birthrate has remained above 10% (March of Dimes, 2024), and The World Health Organization reports that each year, more than 20 million infants worldwide are born weighing less than 2.5 kg who need human milk to improve outcomes and decrease their incidence of necrotizing enterocolitis (WHO, 2023).
In September of 2023, a bipartisan bill, H.R. 5486, was introduced to the House to improve access to pasteurized donor milk. This bill would provide additional funding for Women, Infants, and Children (WIC) to educate on the importance of donor milk and financially support increased access to donor milk. Additionally, 1 million dollars would go towards education for the public on the need for donor milk and awareness about milk banks. Education and access to support for breastfeeding would work to provide the benefits of breastmilk for more infants in the United States (Access to Donor Milk, 2023).
In recent years, there have been formula shortages and recalls and H.R. 5486 would work to provide 3 million dollars for milk banks to respond to a rapid and increased need for donor milk in such situations (Access to Donor Milk, 2023). The recent shortages have come from recalls and supply chain issues; however, the last few years have proven the uncertainty of supply for many food items. The most recent recall affected the preferred brand for WIC and disproportionately affected low-income families (Jung, J., Widmar, N., & Ellison, B., 2023). Although the government has responded in an attempt to mitigate these issues for the future, the most important intervention is to promote breastfeeding and the provision of human milk and thereby decrease reliance on formula (Jung, J., Widmar, N., & Ellison, B., 2023).
When delivering donor milk, the safety of the milk should be paramount, and H.R. 5486 would require the Secretary of Health and Human Services to draft standards for “collecting, processing, handling, transferring, and storing donor milk” (HMBANA, 2023). The Human Milk Banking Association, considered to be the experts on human milk banking, published standards for donor milk banking in 2020. Through their mission statement, they share their belief "...in a world where all infants have access to human milk through support of breastfeeding and use of donor human milk” (HMBANA, 2020). The World Health Organization also acknowledges the importance of human milk for low birth weight infants and recommends provision of mothers' own milk or donor milk where safe and affordable milk banking can be set up (WHO, 2023). Acknowledgment by the WHO is an important milestone for spreading the message of how critical human milk is for all infants, particularly for premature infants.
H.R. 5486, if passed, would be a tremendous step forward for spreading awareness and the availability of human milk for babies in our country. Consider writing your representatives today to support this bi-partisan bill, which will support our patients and families. If you are aware of a parent, family member, or friend with excess human milk, share your local donor human milk bank information for them to consider donating.
References:
Access to Donor Milk of 2023, H.R. 5486, 118th congress. (2023). https://www.congress.gov/bill/118th-congress/house-bill/5486
Centers for Disease Control. (2023). Breastfeeding Benefits Both Baby and Mom. https://www.cdc.gov/nccdphp/dnpao/features/breastfeeding-benefits/index.html#:~:text=Breast%20milk%20antibodies%20help%20protect,against%20certain%20illnesses%20and%20diseases.
Human Milk Banking Association of North America. (2023). HMBANA applauds introduction of legislation which would increase access to donor milk. https://www.hmbana.org/news/blog.html/article/2023/09/21/hmbana-applauds-introduction-of-legislation-which-would-increase-access-to-donor-milk
Jung J., Widmar N., & Ellison B. (2023) The Curious Case of Baby Formula in the United States in 2022: Cries for Urgent Action Months after Silence in the Midst of Alarm Bells. Food Ethics. 2023;8(1):4. doi: 10.1007/s41055-022-00115-1.
March of Dimes. (2024). Prematurity Profile. https://www.marchofdimes.org/peristats/reports/united-states/prematurity-profile
Nationwide (2022). Breastfeeding your premature baby. https://www.nationwidechildrens.org/conditions/health-library/breastfeeding-your-premature-baby
World Health Organization. (2023). Donor human milk for low birth weight infants. https://www.who.int/tools/elena/interventions/donormilk-infants#:~:text=WHO%20Recommendations,or%20can%20be%20set%20up.
January 2024 - It’s a New Year, Consider Advocacy!
Michele A Sweet MS, RN, CCNS
Did you know…a quarter of people quit their New Year’s resolutions during the first week, and close to half by the end of the month? (Fisher, 2023) If you’re still in search of a 2024 goal, how about trying a resolution that helps your community and local or state government? Have you thought about advocacy?
Advocacy is defined as “any action that speaks in favor of, recommends, argues for a cause, supports or defends, or pleads on behalf of others.” (Oxford, 2024) If you are motivated by what is happening in your community or state, or environmental or healthcare issues have you worried, you have already started the advocacy journey.
The 118th Congress began on January 3, 2023, and will end on January 3, 2025. This Congress is one of the most racially and ethnically diverse in history. Additionally, the number of women in Congress is at an all-time high, and the number of openly LGBTQ+ lawmakers is also on the rise. Also of note, 15% (82) are newly elected lawmakers. (Schaeffer, 2023)
How to get started. Advocacy starts with identifying a concern or cause that resonates with you and speaking out in favor of or against it. The first step to getting started is to know your representatives and senators. Some states have held special elections for newly open seats related to retirement or a change in position within the government. Search for your state representatives at house.gov and senators at senate.gov.
Next steps include locating their offices or finding their contact information. You do not have to go to DC to meet them; they are back in their states almost every week and have office hours. Additionally, contact info can be found on their websites, which include email and phone numbers, and how to request an appointment at a local office. Many sites even have a contact form that makes connecting simple.
Not sure what to say to your representative or senator? Start by attending a town hall meeting, or draft an email or scripted phone message. There are many resources for how to connect out there, most notably on the NANN/HPAC webpage. The best advice for your outreach is to share your personal story and concern and be specific. Congress has legislative aides and librarians who provide the facts on pending legislation and search the literature for them. We bring great value as nurses, one of the most trusted professions, by sharing our stories with the people in these roles. (ANA, 2024)
Maybe there’s a particular bill or piece of pending legislature that you are concerned about? Or you might be uncertain if a law passed or who is sponsoring the bill. Search Bills in Congress - GovTrack.us is a bill tracker that also provides details on how many members of Congress have signed onto a bill and if it is bipartisan, with both Democratic and Republican parties sponsoring.
Curious about Congress overall and feel like you need more information? Try perusing the wealth of information at congress.gov. Visit websites and follow your governing leaders on social media to really get to know them and what they stand for. This time next year, we will check back to see if we have persuaded you toward advocacy. We’d like to hear how you got started and about any emails, letters, or phone calls you made to start your new journey. Have questions? Reach out to Michele Sweet, Chair, NANN Health Policy and Advocacy Committee, at This email address is being protected from spambots. You need JavaScript enabled to view it..
References
Batts, Richard. (2023, February 2). Why Most New Year's Resolutions Fail. The Ohio State University @Fisher College of Business.https://fisher.osu.edu/blogs/leadreadtoday/why-most-new-years-resolutions-fail
This email address is being protected from spambots. You need JavaScript enabled to view it.. (2024, January 22) America’s Most Trusted: Nurses Continue to Rank the Highest. American Nurses Association. https://www.nursingworld.org/news/news-releases/2024/americas-most-trusted-nurses-continue-to-rank-the-highest/
Oxford University Press. (2024). https://languages.oup.com/google-dictionary-en/
Schaeffer, Katherine. (2023, February 7). The changing face of Congress in 8 charts. Pew Research Center. https://pewrsr.ch/3jCDX5r
Seddiq, Oma. (2023, January 2) Meet the freshman class: Congress' new members include 13 women of color, the 1st Gen Z lawmaker, and some familiar faces. Business Insider. https://www.businessinsider.com/new-lawmakers-incoming-freshman-class-118th-congress-2022-12
Websites
Find Your Representative | house.gov
Search Bills in Congress - GovTrack.us
October 2023 – Workplace Violence Legislation Update
Katelyn M. Halstead, BSN RN RNC-NIC C-NNIC C-ELBW IBCLC
Nurses have long been at the forefront of creating a safe space for patients and families. The call to advocacy by nursing and the needs of nurses from society are clearly outlined in the American Nurses Association book, Guide to Nursing’s Social Policy Statement: Understanding the Profession from Social Contract to Social Covenant. Conversely, workplace violence against nursing and burnout is rising. The American Nurses Association reports that 84% of registered nurses are experiencing burnout while 42% of nurses believe their employer values their mental health. On a physical scale, 1 in 4 nurses report being physically assaulted in the workplace. The United States Bureau of Labor Statistics finds that healthcare and social service workers are five times more likely to suffer workplace violence injury than any other worker. On a system impact level, nonfatal injuries and illnesses resulting in days off work amongst nurses increased by 291% in 2020. Both personal capacity to cope with workplace stressors and positive improvements in the healthcare system are necessary. In the United States Political realm, change is occurring on an individual and system level at varying degrees of momentum.
The Dr. Lorna Breen Health Care Provider Protection Act or Public Law 117-105, was passed on March 18, 2022. Through Public Law 117-105, The Department of Health and Human Services (HHS) will award grant funding to support mental health and resiliency for healthcare workers. HHS is also obligated to conduct a movement to encourage healthcare workers to seek support and publicize best practices to prevent suicide and improve resiliency. In addition to campaigning, HHS must study and develop policy recommendations. The Government Accountability Office will be reporting the effects of all grants awarded for the efficacy of their interventions.
Doctor Lorna Breen of New York inspired a change in law for all healthcare workers. She was an emergency physician at New York Presbyterian Hospital at the height of the COVID-19 Pandemic. Lorna’s dream since childhood had been to help others as an emergency physician. She was also a daughter, a sister, an aunt, a friend, a fellow healthcare worker and a human being. Dr. Lorna Breen died of suicide on April 26, 2020. She had no risk factors besides being a healthcare worker, specifically a physician. Like Lorna, nurses also share a risk factor for suicide by working in their chosen profession. Pre-pandemic data shows that nurses, specifically female nurses, are 70% more likely than female physicians to die by suicide; two times more likely than the general public.
On a system level, The Workplace Violence Prevention for Health Care and Social Service Workers Act or HR 1195 passed the House of Representatives, but did not pass the Senate before the 117th Convention of Congress adjourned. HR 1195 required the Labor Board to address workplace violence in healthcare, social sectors and other sectors. Interim guidelines would have been issued to protect workers until a final standard was issued within a defined timeline. Currently, Senator Courtney has reintroduced The Workplace Violence Prevention for Health Care and Social Service Workers Act as HR 2663 to the 118th Convention of Congress. The Bill has been referred to the Committee on Education and the Workforce, in addition to the Committees on Energy and Commerce, and Ways and Means. S 1176, The Workplace Violence Prevention for Health Care and Social Service Workers Act was also reintroduced by Senator Tammy Baldwin and is currently referred to the Committee on Health, Education, Labor, and Pensions.
Additionally, HR 2584: The Safety from Violence for Healthcare Employees or SAVE Act was introduced by Representative Larry Bucshon on April 13, 2023. HR 2584 acknowledges the widespread problem of workplace violence preceding the COVID-19 Pandemic as early as 2011. States are and will remain responsible for prosecuting violent crimes under the proposed SAVE Act. However, the argument is made that the states would have increased leverage to protect workers against assault and intimidation with Federal Law enforcement protections and involvement. Federal involvement would allow for teamwork between Federal, State and Local Authorities to investigate and prosecute certain violent crimes. Grant money is proposed to be made available to qualifying healthcare facilities to train staff in de-escalation, specialized self-defense and/or structural protections such as panic buttons or metal detectors. The committee reviewing this Bill is the House Committee on the Judiciary.
A free update on legislation to track progress on bills and an archive of current law can be found at www.congress.gov. Links to contact respective representatives are also available to make certain Nursing voices are heard regarding these important issues.
References
ANA Enterprise. (2022, April 21). Workplace violence in nursing. ANA. https://www.nursingworld.org/practice-policy/work-environment/end-nurse-abuse/workplace-violence/#:~:text=1%20in%204%20nurses%20reported,violence%20may%20be%20much%20higher
Bureau of Labor Statistics, U.S. Department of Labor, The Economics Daily, Nonfatal injuries and illnesses resulting in days off work among nurses up 291 percent in 2020 at https://www.bls.gov/opub/ted/2022/nonfatal-injuries-and-illnesses-resulting-in-days-off-work-among-nurses-up-291-percent-in-2020.htm (visited September 13, 2023)
Creative Commons Attribution-NoDerivatives 4.0 International License. (2023, September 9). About lorna. Dr. Lorna Breen Heroes Foundation. https://drlornabreen.org/about-lorna/
Fowler, M. D. M. (2019). Guide to” ’Nursing’s Social Policy Statement (12th ed., pp. 19-23). American Nurses Association.
H.R.1195 - 117th Congress (2021-2022): Workplace Violence Prevention for Health Care and Social Service Workers Act. (2021, April 19). https://www.congress.gov/bill/117th-congress/house-bill/1195
H.R.1667 - 117th Congress (2021-2022): Dr. Lorna Breen Health Care Provider Protection Act. (2022, March 18). https://www.congress.gov/bill/117th-congress/house-bill/1667
Khammissa, R. A. G., Nemutandani, S., Feller, G., Lemmer, J., & Feller, L. (2022). Burnout phenomenon: neurophysiological factors, clinical features, and aspects of management. The Journal of international medical research, 50(9), 3000605221106428. https://doi.org/10.1177/03000605221106428
Lee, K. A., & Friese, C. R. (2021). Deaths by Suicide Among Nurses: A Rapid Response Call. Journal of psychosocial nursing and mental health services, 59(8), 3–4. https://doi.org/10.3928/02793695-20210625-01
Related Bills - H.R.1195 - 117th Congress (2021-2022): Workplace Violence Prevention for Health Care and Social Service Workers Act. (2021, April 19). https://www.congress.gov/bill/117th-congress/house-bill/1195/related-bills
S.1176 - 118th Congress (2023-2024): Workplace Violence Prevention for Health Care and Social Service Workers Act. (2023, April 18). https://www.congress.gov/bill/118th-congress/senate-bill/1176
S.4182 - 117th Congress (2021-2022): Workplace Violence Prevention for Health Care and Social Service Workers Act. (2022, May 11). https://www.congress.gov/bill/117th-congress/senate-bill/4182
Text - H.R.1195 - 117th Congress (2021-2022): Workplace Violence Prevention for Health Care and Social Service Workers Act. (2021, April 19). https://www.congress.gov/bill/117th-congress/house-bill/1195/text
Text - H.R.1667 - 117th Congress (2021-2022): Dr. Lorna Breen Health Care Provider Protection Act. (2022, March 18). https://www.congress.gov/bill/117th-congress/house-bill/1667/text
Text - H.R.2584 - 118th Congress (2023-2024): SAVE Act. (2023, April 13). https://www.congress.gov/bill/118th-congress/house-bill/2584/text
Text - H.R.2663 - 118th Congress (2023-2024): Workplace Violence Prevention for Health Care and Social Service Workers Act. (2023, April 18). https://www.congress.gov/bill/118th-congress/house-bill/2663/text
July 2023 – A Call to Action: Black Maternal Health Momnibus 2023
Lisa Davenport, DNP, RN, RNC-NIC
Maternal mortality is on the rise in the United States with 32.9 deaths per 100,000 births in 2021, which is a 40% increase over the previous year (Centers for Disease Control, 2023a). Other developed nations, such as New Zealand and Norway, sustain a significantly lower maternal mortality rate, reporting fewer than three per 100,000 births (OECD, 2023). In 2022, the CDC released data showing that 84% of these maternal deaths in the US are preventable (Centers for Disease Control, 2022). Amongst our nation, there stands a wide variation in maternal mortality rates, with Mississippi reporting an alarming 82.5 per 100,000 births and California reporting 9.7 per 100,000 births (Centers for Disease Control, 2023b). Along with the shocking rise in overall maternal mortality in our country, black mothers in the United States are three times more likely to die from pregnancy related issues than white mothers (Centers for Disease Control, 2023c). This alarming health disparity can be attributed to multiple factors including underlying health conditions, bias, and social determinants of health however, money and resources need to be allocated to close this gap.
The recent release of maternal mortality statistics prompted senators to introduce Senate Bill S.1606, known as Black Maternal Health Momnibus 2023 on May 15, 2023 in honor of Mother’s Day. S.1606 aims to “to end preventable maternal mortality, severe maternal morbidity, and maternal health disparities in the United States” (Black Maternal Health Momnibus, 2023). The tenets of the bill work to improve the federal maternal health structure with the creation of a task force including the highest levels of government leadership to provide support to eliminate preventable maternal deaths. The 2022 Maternal Care Report from the March of Dimes reported increasing Maternal Care Deserts in the US with 6.9 million women and 500,000 births having low or no access to care in our country. Access to quality maternal care is critical for outcomes and Momnibus would aim to remove barriers to care, provide resources to patients to address basic needs such as food and housing, address environmental concerns, collaborate with healthcare organizations to improve outcomes, and address domestic abuse in pregnancy. A needed and progressive action by the bill would extend WIC benefits from 1 year to 2 years as well as recommendations of extended breastfeeding support to 2 years.
Healthcare providers have the duty to create awareness, mitigate unconscious bias, and address social determinants of health to serve all patients. Under the Momnibus bill, grants would provide funds to reduce bias and racism in healthcare settings with the provision of education and care collaboratives. With the provision of resources, hospitals would be required to post mitigation strategies publically to allow the consumer to choose healthcare organizations based on the foundation of respectful maternal care. In 2021, the Association of Women’s Health and Neonatal Nurses (AWHONN) created a tool kit on the creation of respectful maternity care. This tool kit is a launching pad for organizations to provide respectful care to every patient. Additionally, under Momnibus, 15 million dollars of funding annually would go towards reducing maternal health disparities in veterans with the provision of enhanced maternal care coordination. Diversity in the maternal care workspace is supported via Momnibus with resources to recruit and train a diverse workforce, which is willing to practice in underserved areas. Maternal mental health is also part of this comprehensive package to ensure that the mothers’ physical and emotional needs are being met.
The MOMNIBUS bill if approved stands to change the face of maternal care by addressing social determinants of health and reducing disparities specifically for black women. Consider writing your senators or signing on to support maternal health outcomes with other organizations like March of Dimes.
References
Association of Women’s Health and Neonatal Nurses. (2021). Respectful maternal care implementation
toolkit. https://www.awhonn.org/respectful-maternity-care-implementation-toolkit/
Black Maternal Health Momnibus, S.1606, 118th Congress. (2023). https://www.congress.gov/bill/117th-congress/house-bill/959
Centers for Disease Control. (2022). Pregnancy-Related Deaths: Data from Maternal Mortality Review Committees in 36 US States, 2017–2019. https://www.cdc.gov/reproductivehealth/maternal-mortality/erase-mm/data-mmrc.html
Centers for Disease Control. (2023a). Maternal mortality rates in the United States, 2021. https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2021/maternal-mortality-rates-2021.htm
Centers for Disease Control. (2023b). National Vital Statistics Reports: Births: final data for 2021. https://www.cdc.gov/nchs/data/nvsr/nvsr72/nvsr72-01.pdf
Centers for Disease Control. (2023c). Working together to reduce black maternal mortality. https://www.cdc.gov/healthequity/features/maternal-mortality/index.html
March of Dimes. (2021). Maternal death and pregnancy related death. https://www.marchofdimes.org/find-support/topics/miscarriage-loss-grief/maternal-death-and-pregnancy-related-death #:~:text=About%20700%20moms%20die%20each,complications%20during%20or%20after%20pregnancy.&text=We%20call%20this%20a%20health%20disparity%20(difference).
March of Dimes. (2022) Maternal care desert report. https://www.marchofdimes.org/maternity-care-deserts-report
Organization for Economic Cooperation and Development. (2023). Health status: maternal and infant mortality. https://stats.oecd.org/Index.aspx?ThemeTreeId=9
May 2023 - A Call to Action: PREEMIE Reauthorization Act of 2023
Taryn M. Edwards, MSN, APRN, NNP-BC
The second leading cause of infant death is preterm birth, along with low-birth-weight infants (Centers for Disease Control, 2022a). In 2021, there were 383,082 preterm births, representing 10.5% of live births (Centers for Disease Control, 2022b). The overall preterm birth grade in the United States is D+, without improvement since 2011 (March of Dimes, 2022). In fact, from 2020 to 2021, the preterm birth rate increased by 4% (Centers for Disease Control, 2022b). Certain areas of the United States, majority of southern states, have a higher incidence of preterm birth. In addition, certain racial/ethnic groups have a higher incidence of preterm birth, including Black, American Indian/Alaska Native, and Hispanic. The cause of preterm births is sometimes unknown or can occur due to risk factors, which includes multiple pregnancies, infections, and chronic conditions such as diabetes and high blood pressure, that often lead to long-term health problems, including developmental delay, chronic respiratory problems, and vision and hearing impairment. Preterm birth and the ongoing care needed impacts families emotionally and financially, with an annual societal economic cost (medical, education, and lost productivity) estimated at $25.2B (Waitzman, Jalali, & Grosse, 2021).
In 2006, Congress passed the original PREEMIE Act (P.L. 109-450), expanding research and developing an agenda aimed at reducing preterm birth and its consequences. The Act was reauthorized in 2018 (S. 3029/H.R. 6085), renewing the U.S.’s commitment to address preterm birth through federal research, promoting known interventions, and promoting community initiatives. At the end of 2023, research and programs made possible by the PREEMIE Act will be put at risk when approval for these programs ends. On May 12th, Sen. Michael Bennet (D-CO), Sen. John Boozman (R-AZ), Rep. Burgess (R-TX), Rep. Eshoo (D-CA), Rep. Miller-Meeks (R-IA), Rep. Kelly (D-IL), Rep. Jen Kiggans (R-CA), and Rep. Lisa Blunt Rochester (D-DE) reintroduced the PREEMIE Reauthorization Act. Key provisions include renewal of the Centers for Disease Control and Prevention (CDC) research and programs on preterm birth, which includes improved tracking of national data; reauthorization of the Health Resources and Services (HHS) Administration activities of promoting healthy pregnancies and preventing preterm births; provide for a new study on the costs, impact of social factors, gaps in public health programs that lead to prematurity, and calls for HHS to make recommendations to prevent preterm birth; and establishment of an entity in the Department of Health and Human Services to coordinate all federal activities and programs related to preterm birth, infant mortality, and other adverse birth outcomes. Supporting reauthorization will ensure that these lifesaving programs continue.
NANN, NANNP (National Association of Neonatal Nurse Practitioners, the APRN division of NANN) and HPAC (the NANN Health Policy Advocacy Committee) are urging you to contact your representatives by utilizing the March of Dimes form here: https://p2a.co/mogVH96. Please share any personal stories in this automated email format to further display the importance of ongoing funding for the PREEMIE Reauthorization Act of 2023. Share this link on your social media platforms, in addition to family and friends.
References
Centers for Disease Control and Prevention. (2022a, June 22). Infant mortality. Retrieved May 22, 2023, from https://www.cdc.gov/reproductivehealth/maternalinfanthealth/infantmortality.htm.
Centers for Disease Control and Prevention. (2022b, November 1). Premature birth. Retrieved May 22, 2023, from https://www.cdc.gov/reproductivehealth/features/premature-birth/.
March of Dimes. (2022, November 15). 2022 March of Dimes Report Card for United States. Retrieved May 19, 2023, from https://www.marchofdimes.org/peristats/reports/united-states/report-card.
March of Dimes. (2023). Preemie Reauthorization Act. Retrieved May 19, 2023, from https://www.marchofdimes.org/sites/default/files/2023-05/PREEMIE_Reauthorization_Act_Issue_brief_v7.pdf.
Waitzman, N.J., Jalali, A., & Grosse, S.D. (2021). Preterm birth lifetime costs in the United States in 2016: An update. Seminars in Perinatology, 45(3):151390. doi: 10.1016/j.semperi.2021.151390. PMID: 33541716.
April 2023 - Diversity in the Neonatal Nursing Workforce
Michelle Ferrant, DNP, ACCNS-N, RNC-NIC, CBC, CPLC
We are currently amidst a crisis in healthcare in the United States. According to the March of Dimes (MOD) 2022 Report Card, the U.S. preterm birthrate has hit a 15-year high, earning a D+ grade (March of Dimes, 2022). The crisis expands beyond the neonatal population to maternal and neonatal deaths, also on the rise (March of Dimes, 2022). Among these statistics, the crisis is disproportionately affecting black pregnant and expecting mothers and their babies (March of Dimes, 2022). As neonatal nurses, this data concerns us and directs our attention on how to address the disparities in neonatal care.
While there are many complex components contributing to the disparity, attention should be paid to the workforce caring for our patients. As neonatal nurses, we are the largest healthcare provider interacting and providing care for neonates. Working toward achieving racial and ethnic composition that mirrors the population we serve contributes to our workforce. According to data from the 2020 U.S. Census, 60% of the population self-identified as White/Caucasian, 12% as Black and 19% as Latinx (US Census Bureau, 2022). The proportion of birthing people is like the overall census data and has been reported as 48.5% being racial and ethnic minorities of which 14% were non-Hispanic Black women (Hamilton et al., 2022). The overall nursing workforce is 81% White/Caucasian and 7% Black according to the 2020 survey (Rosseter, 2022). A recent study on the neonatal nurse practitioner students and faculty workforce also mirrors these statistics with underrepresented minorities in discordance with the patient population (Newberry & Bell, 2023). Nearly half of our patients are racial or ethnic minorities, but most of the nurses and healthcare professionals who treat them will be white.
Having gaps this significant in the demographics of the population we serve, and clinicians providing care, can have critical consequences for both care delivery and health outcomes (Kozhimanil et al., 2021). Lack of diversity among the healthcare clinicians has been linked to worse health outcomes for underrepresented populations (Kozimanil et al., 2021). NANN’s advocacy agenda states that all infants, regardless of race, parental economic or educational status, or geographical area should receive equitable and quality healthcare (NANN, 2022). When discussing inequities in healthcare for racial and ethnic minorities, the social determinants of health are also influencing factors (US Department of Health and Human Services, 2023; Litt et al., 2020). The US history of racial segregation and subsequent neighborhood deprivation that has been associated with poor health outcomes is then further compounded when the healthcare workforce does not have adequate diversity (Litt et al., 2020).
As neonatal nurses, what can we do to address the diversity issue in our workforce? There are ways to increase the diversity of neonatal nurses at the institutional, local, state, and federal levels. In your institution, you can advocate for, if not already in place, Diversity, Equity, and Inclusion (DEI) practices and have processes in place to look at the demographics of your patient population and your clinical staff. Many academic nursing leaders are addressing diversity and instituting initiatives that foster DEI. How many of us know what our local academic institutions are doing? Collaborating with our local academic leaders to determine what, if any, actions are being taken is a step in the right direction to increasing the diversity, inclusiveness and allyship of the nursing student population that will soon be a part of our workforce. Some leading nursing schools are on the forefront of addressing student population diversity. One of the nation's largest nursing schools, Chamberlin University, has created a research-based framework to advance efforts and create a more diverse pool of students entering the profession (Davis, 2023). Nursing school diversity begins before admission; partnering with K-12 educations systems for career discussions and mentorship and including students from diverse areas that may differ from typical their typical acceptance pool can increase student diversity (Davis, 2021).
On a federal level, there have been several bills introduced that are written to address health disparities and healthcare workforce diversity. The Black Maternal Momnibus Act of 2021, which has provisions for actions to both grow and diversify the maternal health workforce, was introduced into the House and Senate, but they have stalled after being referred to their respective committees. There is also the Health Equity and Accountability Act of 2022, which also directs support of healthcare workforce diversity as well as requiring detailed reporting of demographic and health disparity data, aiding in the creation of initiatives at local levels. It also has been introduced but has not advanced since being referred to a House subcommittee and a Senate committee. Contacting your representatives is a vital and critical component to our governmental process; hearing your personal concerns and voice is how government works.
Even small efforts can make an impact – recognizing the issue of diversity in our neonatal nursing workforce is the first step, and working toward a neonatal nursing workforce that reflects our patient population will result in improved neonatal outcomes.
Learn More
Black Maternal Health Momnibus Act of 2021: H.R. 959 (2021) https://www.congress.gov/bill/117th-congress/house-bill/959
Black Maternal Health Momnibus Act of 2021: S.346 (2021) https://www.congress.gov/bill/117th-congress/senate-bill/346
Health Equity and Accountability Act of 2022: H.R. 7585 (2022) https://www.congress.gov/bill/117th-congress/house-bill/7585
Health Equity and Accountability Act of 2022: S.4486 (2022) https://www.congress.gov/bill/117th-congress/senate-bill/4486
References
Davis, C. (2021, December). 3 nursing schools that have put diversity and inclusion at the forefront. HealthLeaders Media. Retrieved March 31, 2023, from https://www.healthleadersmedia.com/nursing/3-nursing-schools-have-put-diversity-and-inclusion-forefront
Davis, C. (2023, January 31). Lack of racially diverse NPS in neonatal icus creates 'glaring health disparities'. HealthLeaders. Retrieved March 2, 2023, from https://www.healthleadersmedia.com/nursing/lack-racially-diverse-nps-neonatal-icus-creates-glaring-health-disparities
Hamilton, B. E., Martin, J. A., & Osterman, M. J. K. (2022). Births: Provisional Data for 2021. Vital Statistics Rapid Release.
Kozhimannil, K. B., Almanza, J., & Hardeman, R. (2000). Racial and Ethnic Diversity in the Nursing Workforce: A Focus on Maternity Care. Policy, Politics, & Nursing Practice, 22(3), 170–179. https://doi.org/10.1177/15271544211005719
Litt, J. S., Fraiman, Y. S., &; Pursley, D. W. M. (2020). Health equity and the social determinants: Putting newborn health in context. Pediatrics, 145(6). https://doi.org/10.1542/peds.2020-0817
March of Dimes. (2022, November 15). March of dimes 2022 report card shows U.S. prete15rm birth rate hits 15-year high rates increase for women of all races, earning Nation D+ grade. March of Dimes. Retrieved March 2, 2023, from https://www.marchofdimes.org/about/news/march-dimes-2022-report-card-shows-us-preterm-birth-rate-hits-15-year-high-rates#:~:text=The%20report%20shows%20that%20the,as%20compared%20to%20White%20women
National Association of Neonatal Nurses. (2022). NANN Advocacy Agenda (2022) - National Association of Neonatal Nurses. NANN Advocacy. Retrieved March 2, 2023, from https://nann.org/uploads/Updated_NANN_Advocacy_Agenda_2022.pdf
Newberry, D. M., & Bell, T. (2023). Racial and Ethnic Composition of Neonatal Nurse Practitioner Faculty and Students in the United States. Advances in Neonatal Care, 10-1097.
Rosseter, R. (2022, September). Fact Sheet: Enhancing Diversity in the Nursing Workforce. American Association of Colleges of Nursing: The Voice of Academic Nursing. Retrieved March 2, 2023, from https://www.aacnnursing.org/news-information/fact-sheets/enhancing-diversity
US Census Bureau. Race and Ethnicity in the United States: 2010 Census and 2020 Census. Suitland, MD: US Census Bureau, 2022. Retrieved March 2, 2023, from Race and Ethnicity in the United States: 2010 Census and 2020 Census
U.S. Department of Health and Human Services. (2023). Neighborhood and built environment. Neighborhood and Built Environment - Healthy People 2030. Retrieved March 31, 2023, from https://health.gov/healthypeople/objectives-and-data/browse-objectives/neighborhood-and-built-environment
February 2023 - Providing Informed Care to LGBTQ+ Families
Raymond K Riley, BSN, RNC-NIC
He / Him / His
As nurses, it is our ethical responsibility to care for our patients and their families. All patients and their families are unique. It is very important for us to provide non-judgmental care that is free of bias to support the families and ensure we build a trustworthy relationship. When you’re caring for someone’s baby, trust is vital throughout the process and especially when it comes to the education needed to maintain health and success after discharge. Now that the importance of a non-judgmental, trusting relationship between the nurse, patient, and family has been established, how do we get there?
First, let’s make sure we have a good handle on a few current terms and a few outdated terms. A person’s gender or gender identity is defined as one’s innermost concept of self as male, female, a blend of both, or neither. This is how an individual perceives themself and how they refer to themself. A common misconception is to assume that the sex assigned at birth, which is usually determined by a medical professional, also determines gender identity. The announcement of the sex of an infant is based on external genitalia and that does not always align with how an individual will identify themselves throughout their life (HRC, 2023). It is important to know the difference and to respect an individual’s identity.
Another pool of terminology to be aware of surrounds pronouns. This ties into someone’s gender identity. A great way to open that conversation up is to identify your pronouns verbally or list your pronouns on your badge or in your email signature. That behavior invites others to share their pronouns as well by creating an environment of inclusion. The term “preferred pronouns” is now considered outdated as your identity is not a preference, it is a very important part of who you are. Someone does not prefer to identify as a woman, they identify as a woman. When asking someone about or addressing this topic, it is completely acceptable to just say “pronouns” (GLSEN, 2023).
When you walk into a room or approach a bedside, especially for the first time, leave your assumptions behind. No one wants to mistakenly call a baby’s mother “grandma”, and that same awkward and potentially offensive mistake applies to assuming how someone identifies. This can feel like a minefield at times. You don’t want to say the wrong thing or assume the incorrect situation, and sometimes that leads us to silence or even offending the family after all. One great way to avoid this is to just ask. By introducing yourself in a warm and open manner, you’re opening the door for a positive interaction. Then, by asking the right questions, you’re enabling the family to self-identify and teach you about themselves. You might want to ask questions like, “How are you related to the baby?” or “How would you like to be addressed?” When you ask an open-ended question, you have opened the channels of communication for that family to tell you about themselves and what is important to them. If you have a baby that has same-sex parents, allow them to “name” themselves. In our practice you might have a patient with two mothers that want to be “Mom” and “Mommy”. You could also have two fathers that want to be “Dad” and “Papa”. In order to find out, we just have to ask.
It can also be helpful to keep yourself informed of the political climate in your region/state. There is legislation being introduced all the time that limits and expands LGBTQ+ rights. That doesn’t always inspire confidence in the system for these families. There may be a lot of apprehension about how they will be received or treated in the hospital, especially if the system has failed them before. For example, Congress recently passed the Respect for Marriage Act. This piece of legislation protects any marriage that was done in a state where it was legally certified, if another state were to make that same marriage illegal. Basically, if a same-sex couple is married in state A, and then they move to state B where same-sex marriage is made illegal, state B has to honor their marriage as legitimate (Respect for Marriage Act, 2022). Keeping yourself informed of the political climate and how it may affect your patients and their families is always a good rule of thumb.
As a profession we have done and continue to do amazing things every day. Let’s make 2023 a year of acceptance for all our patients and their families and continue to be the change we want to see in the world.
Glossary of Terms. Human Rights Campaign. (2023). Retrieved January 3, 2023, from https://www.hrc.org/resources/glossary-of-terms.
Pronouns: A Guide from GLSEN. GLSEN. (2023). Retrieved January 4, 2023, from https://www.glsen.org/activity/pronouns-guide-glsen.
Respect for Marriage Act, Public Law 117-228. (2022). https://www.congress.gov/117/plaws/publ228/PLAW-117publ228.pdf.
October 2022 - Why should nurses care about elections?
Tommie Farrell, BSN
We are approaching the midterm elections which are set for November 8. There are so many healthcare issues and policies that impact our practice, our patients, and the overall health of our nation. Many of us only see the election cycle as "politics" and do not think of how pivotal our votes are toward impacting healthcare. There are over 4 million nurses who have the voting power to impact change. But do you know the issues for which you are voting? What is important to us, as healthcare influencers?
I encourage you to examine issues locally, statewide, and nationally. It is important to research and do your homework. Paying attention to the "noise" of social media and TV commercials is difficult and often misleading and dangerous.
As healthcare professionals and stewards, we are charged with the health and welfare of our patients. We can only do this by putting in the work. Putting in the work involves researching the candidates, encouraging everyone to vote, contacting candidates on why your voice matters and why healthcare matters to everyone. Take the time to call candidates offices, state your concerns as an RN, and remind them what healthcare should look like (they may need education). Give examples from your own practice that impacts the decisions they make. These are significant ways to become a changemaker, especially when 4 million plus are doing it! A great piece of advice when advocating is to focus on key issues and tie them to your community and practice when talking to local candidates.
The ANA calls for nurses to participate in health policy. Recently the AMA as well as NIH have acknowledged that voting is a social determinant to health. Healthcare experiences are often shaped by healthcare policy and according to Vot-ER, there are an estimated 51 million unregistered voters (often "at risk" people, who won't be represented). We need to find ways to impact voter registration.
Here are the health policy issues on the ballot for the midterms:
- Expansion of the ACA
- Medicare Payment Reductions
- The Momnibus Bill-Black Maternal Health Act (key issues for our patients, including expanded postpartum care and Medicaid complement)
- Health Equity/Improving Data-particularly as it impacts healthcare deserts, rural areas, POC, LGBTQ, people who are living below the poverty line and other struggling communities
- Surprise Billing Implementation
- Public Health Legislation-(response to pandemics, supply chain, shortages)
- Cures 2.0 (multiple issues- telehealth, access to research, therapeutics)
- Reproductive Rights
- Drug Pricing (e.g., Insulin) and access to other lifesaving medications
- Environmental and Climate Justice
- Looking at the issues, they intersect with NANN's Advocacy Agenda. These include Healthcare Disparities, Covid-19 impacts, Mental Health, Nursing Workforce, Environmental/Climate issues, Paid Family Leave, and Access to Nutrition and Education surrounding Human Milk provisions.
Elections are essential to our nursing practice and NANN encourages you to participate in shaping the healthcare for our patients and our nation. Your VOICE impacts healthcare policy.
Resources
Brown CL, Raza D, Pinto AD. Voting, health and interventions in healthcare settings: a scoping review. Public Health Rev. 2020 Jul 1;41:16. doi: 10.1186/s40985-020-00133-6. PMID: 32626605; PMCID: PMC7329475.
Firth S. Washington Correspondent, MedPage Today AMA Acknowledges Voting Is a Social Determinate of Health. MedPage Today. 2022 June 14.
Health.gov, Healthy People 2030.
Holland & Knight Healthcare Blog, 2022 Congressional Outlook and Top 10 Federal Health Policy Issues to Watch, 2022, January 6.
nursingworld.org -ANA, RNAction.
USA.gov.
Vot-ER.org.
Yagoda N. Addressing Health Disparities Through Voter Engagement. Ann Fam Med. 2019 Sep;17(5):459-461. doi: 10.1370/afm.2441. PMID: 31501209; PMCID: PMC7032920.
September 2022 - A Look at Providing Human Milk Over the Years
Michele A. Sweet MS RN ACCNS-Neo
World Breastfeeding Week was first celebrated in 1992 with declarations and legislation in more than 120 countries to “protect, promote, and support” breastfeeding.5 Breastfeeding was recognized as “wet nursing” from 2000BC until the 20th century; this was a means, moreover, need to feed babies back then.11 Today we celebrate world breastfeeding the first week of August; with the month of August then declared National Breastfeeding Awareness Month. National Indigenous Milk Medicine, Asian American Native Hawaiian and Pacific Islander Week, and Black Mothers Breastfeeding Week theme observations then follow.8
Breastfeeding rates have gone from 2/3 of women providing human milk in the early 1900’s, to declines of 22% initiation rates and inclines to 70% through the mid 70’s to late 90’s.15 We have learned socioeconomic, cultural and education status of the lactating parent additionally impacts breastfeeding rates. A more well-off, paid for leave parent has shown longer term breastfeeding rates than those of the less-educated and poorer income status in the US.9 Additionally those supported to breastfeed have longer term success feeding at 6 months than those without support or resources.9,10 Breastfeeding became a status symbol at one point defined as a luxury over the necessity for the baby to feed and receive the benefits of their parents human milk.9 This group knows best the science, growth, and impact of a lactating parent feeding their milk to their baby.
Lactating parents need our help, and the support of government and family agencies to be successful and continue providing their milk outside of the hospital.10 We learned in the past decade the importance of breastfeeding within the first hour of a newborn’s life for both c-section and vaginal deliveries. With breastfeeding an established custom from the 20th century to today, how do we continue to give our support? Established Skin to Skin, trained healthcare workers, supplementation w/ breastmilk, and Paid Family Leave are a few of those ways.9
NANN Healthcare Policy and Advocacy Committee is dedicated to improve outcomes for our neonates and their families supporting Paid Family Leave, Nutrition, Direct Provision of Human Milk, and Disparities Within Neonatal Care.6 A Healthy People 2030 goal is to increase the percent of infants breastfed exclusively for six months to 42.4%.1
With headlines stating parents are now “forced” to consider breastfeeding related to the formula shortage, our nation falls into a “crisis” to find ways to feed their babies formula.4 President Joe Biden signed the bipartisan Access to Baby Formula Act into law today, making sure there was government control for formula and enacted Operation Fly Formula, to bring safe and regulated international formula to the USA.12
My hopes for our neonatal population next time would be headlines reading: “Breastfeeding Alternatives are running low, see ways to ramp up your breastmilk supply.” We have accomplished much, with more to do regarding our breastfeeding rates, cultural norms and socioeconomic impacts today. The CDC Breastfeeding Report Card states “Among infants born in 2019, most (83.2%) started out receiving some breast milk, and 78.6% were receiving any breast milk at 1 month.”3 If you are not certain how your state performs, and their legislation to support breastfeeding, then check out the https://www.cdc.gov/breastfeeding/data/reportcard.htm website to see how your state report card measures up, and the work to be done.
References
1. America's Health Rankings analysis of CDC, Breastfed. United Health Foundation, AmericasHealthRankings.org, accessed 2022. https://www.americashealthrankings.org/explore/health-of-women-and-children/measure/breastfed/state/U.S.
2. Black Mother’s Breastfeeding Association. (Extracted 9/11/2022).
https://blackmothersbreastfeeding.org/
3. Center for Disease Control and Prevention. (August 31, 2022). Breastfeeding Report Card, United States, 2022. https://www.cdc.gov/breastfeeding/data/reportcard.htm
4. Goodman, Brenda. (August 2, 2022). Baby formula shortage is easing for many, but it still isn't over. CNN Health.
https://www.cnn.com/2022/08/02/health/baby-formula-shortage-update/index.html
5. Medela. Extracted on 9/10/2022). Why Do We Celebrate World Breastfeeding Week? https://www.medela.com.au/breastfeeding/blog/breastfeeding-lifestyle/why-do-we-celebrate-world-breastfeeding-week.
6. National Association of Neonatal Nurses website: www. http://nann.org/about/advocacy
7. National Institute for Childrens Health Equality. (Extracted 9/11/2022).
https://www.nichq.org/campaign/national-breastfeeding-safe-sleep-month-2022
8. National WIC Breastfeeding Week. (Extracted 9/11/2022).
https://wicworks.fns.usda.gov/resources/national-wic-breastfeeding-week#Other%202021%20Breastfeeding%20Week%20Observations
9. Purtill, Corrine, Kopf, Dan. (Published July 23, 2017Last updated July 20, 2022). FROM OUR OBSESSION, The Art of Parenting. https://qz.com/1034016/the-class-dynamics-of-breastfeeding-in-the-united-states-of-america/
10. Selim, Leah. (extracted on 9/9/2022). Breastfeeding from the first hour of birth: What works and what hurts. https://www.unicef.org/stories/breastfeeding-first-hour-birth-what-works-and-what-hurts
11. Stevens,Emily, Patrick, Thelma E. and Pickler,Rita. A History of Infant Feeding. J Perinat Educ. 2009 Spring; 18(2): 32–39. doi: 10.1624/105812409X426314 Extracted on 9/10/2022 Copyright © A Lamaze International Publication. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2684040/
12. United States Senate Committee on Agriculture, Nutrition, & Forestry. (May21st, 2022). President Biden Enacts Bipartisan Law to Address Baby Formula Shortage.
https://www.agriculture.senate.gov/newsroom/dem/press/release/president-biden-enacts-bipartisan-law-to-address-baby-formula-shortage
13. Vazquez, Maegan. (May 18, 2022). Biden invokes Defense Production Act to address infant formula shortage, among other actions. https://www.cnn.com/2022/05/18/politics/biden-defense-production-act-baby-formula/index.html
14. World Alliance for Breastfeding Action. (Extracted on 9/10/2022). Step up for Breastfeeding Educate and Support. https://worldbreastfeedingweek.org/
15. Wright, Anne L., Schanler, Richard J. The Resurgence of Breastfeeding at the End of the Second Millennium, The Journal of Nutrition, Volume 131, Issue 2, February 2001, Pages 421S–425S, https://doi.org/10.1093/jn/131.2.421S
July 2022 Bonus - Mental Health a Priority for Nurses
Julie Williams, DNP CRNP NNP-BC
One in five adults in the United States experience mental illness each year (National Alliance on Mental Illness, 2022). In 2020, 14.2 million (1 in 20) U.S. adults experienced serious mental illness (SMI) (National Alliance on Mental Illness, 2022). According to the National Institute of Mental Health, SMI is characterized by a mental, behavioral, or emotional disorder which interferes with one’s major activities. Individuals experiencing mental illness often experience physical ailments, including cardiovascular disease, respiratory illnesses, and diabetes among other conditions. Symptoms related to increased stress, exhibited as headaches, anxiety, and feelings of overwhelm may also be experienced.
In April 2020, Dr. Lorna Breen, an emergency room physician at New York Presbyterian, died by suicide after several weeks of providing care for COVID-19 positive patients during the first wave of the pandemic. Dr. Breen’s death highlighted concerns regarding the care of the frontline provider. Nurses as front-line providers were experiencing high stress and burnout prior to the pandemic. The mental toll experienced from the increased patient demand, staffing shortages and increased responsibility has been classified as trauma. In a review of the psychological impact of epidemics/pandemics on healthcare workers, as much as 73% experienced post-traumatic stress symptoms. Ten to forty percent of the surveyed group experienced symptoms for one to three years post pandemic (Preti, Di Mattei, Perego, et. al., 2020).
The recognition, acknowledgement and treatment of symptoms are essential to the protection of one’s mental health. Self-care is important to maintain and improve one’s mental health. Activities including regular exercise, healthy and regular meals, prioritizing sleep, and the adoption of relaxation techniques like meditation should be a part of every nurse’s daily regimen. Nurses should not wait until symptoms are overwhelming. Finally, employers should provide resources for their staff experiencing stress and burnout.
Additional Mental Health Resources
NIMH: Caring for Your Mental Health
CDC: Stress and Coping Resources
Suicide hotline: 988
Bibliography
National Alliance on Mental Illness. (2022). Mental Health by the numbers | NAMI: National Alliance on Mental Illness. Retrieved from https://nami.org/mhstats
Preti, E., Di Mattei, V., Perego, G. et al. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr Psychiatry Rep 22, 43 (2020). https://doi.org/10.1007/s11920-020-01166-z
July 2022 - Environmental Justice and Climate Impacts
Tommie Farrell, BSN RNC
Each year, the Health Policy and Advocacy Committee (HPAC) reviews the HPAC agenda. The agenda reflects the interests of our organization, what would be important for our practice in Neonatology as well as current issues that impact our practice. Often, we agree to leave an item “as is” or in more recent years, we’ve edited or added critical items as noted in the inclusion of the Covid 19 and Healthcare Disparities items due to the impact on health care, policy and our practice.
This year, the committee chose to add “Environmental Justice and Climate Impacts” to the agenda. While it may seem unusual to include this, it is an important part of caring for our patients, as well as educating our present and future workforce. Nurses are ideally suited to address this. Our goal has always been to optimize health at every part of our patient’s development. In order to do that, we must work toward fair and equitable treatment of all people, address environmental and climate issues within this context, recognizing that this is a nursing advocacy role that should be a part of our practice.
Nursing education and standards of nursing practice require that nurses know how to reduce exposures to environmental health hazards (ANA).
In 1995, the Institute for Medicine report, Nursing, Health, and the Environment, clearly stated that environmental health was an important part of nursing practice. It was not clear, at the time, how it would be included in nursing education or practice. Soon after, The Alliance of Nurses for Healthy Environments (ANHE) was formed. It is the only national nursing organization with the sole purpose of combining health and the environment. NANN is actively involved with this group through monthly meetings and collaborates with ANHE when legislation is considered for climate, environment and health issues.
By definition, “Environmental Justice (EJ) is the fair treatment and meaningful involvement of all people regardless of race, color, national origin, or income with respect to the development, implementation and enforcement of environmental laws, regulations and policies”. (EPA)
“People throughout the United States face climate change-related health risks, but some of us will feel the effects earlier and more severely. Groups at increased risk include those with low income, some communities of color, immigrant groups (including those with limited English proficiency), Indigenous peoples, children and pregnant women, older adults, vulnerable occupational groups, persons with disabilities, and persons with preexisting or chronic medical conditions.” (CDC)
“Environmental factors do play an important role in maternal health. They make an important contribution towards placental problems like low birth weight, intrauterine growth restriction, as well as have long term effects on neuronal and behavioral development in adult life.” (NIH)
How we incorporate this into our practice will determine outcomes. Our hope is to start with small but significant steps. Over time, the HPAC committee will look for ways to raise awareness of issues that directly impact our patients and families. Nurses, alone, may not feel that they can impact global and environmental issues. However, we own responsibility to change what we can through small but significant action.
Identifying climate change and environmental pollution as a factor in poor health outcomes is our first step. This is critical in areas where health care disparities already exist. There are several ways to get involved on this topic:
- Commit to raising awareness, education and sharing what we know.
- Incorporate our awareness into action by bringing it into our practice.
- Engage with other organizations (ANHE) to investigate and act on how we can change the trajectory of health outcomes related to environmental toxins and climate change.
- Engage your elected officials, keeping in mind that they depend on us, the nursing community, to guide and influence policy.
- NANN is committed to raising awareness, educate and engage in the conversation, to improve outcomes. We invite you to share your experiences, add to the MyNANN conversation, share information to elevate awareness, and challenge your colleagues to do the same.
References
Triche, E. W., & Hossain, N. (2007). Environmental factors implicated in the causation of adverse pregnancy outcome. Seminars in perinatology, 31(4), 240–242.
https://doi.org/10.1053/j.semperi.2007.07.013
https://www.epa.gov/environmentaljustice
HEALTH, C. O. E. (2015). Global Climate Change and Children's Health. Pediatrics, 136(5), 992-997.
https://health2016.globalchange.gov/climate-change-and-human-health
Leffers J, McDermott-Levy R, Smith CM, Sattler B. Nursing education's response to the 1995 Institute of Medicine Report: Nursing, Health, and the Environment. Nurs Forum. 2014 Oct-Dec;49(4):214-24. doi: 10.1111/nuf.12072. Epub 2014 Jan 8. PMID: 24397834.
Resources
Alliance of Nurses for Healthy Environments
2901 Shepherd Street Mount Rainier, MD 20712
240.753.3729
This email address is being protected from spambots. You need JavaScript enabled to view it.
March 2022 - Advocacy and the Internet
Julie Sundermeier, DNP APRN-NP NNP-BC
Over the past few decades, internet access has changed the way we gain knowledge, communicate, and conduct our lives. Search engine queries instantly provide answers and information. Smart phones are utilized for video conferencing, messaging, scheduling, photography, and so much more. Podcasts and blogs cover news and a variety of other topics. And of course, there are many social media platforms used for virtual networking that, for a vast majority, has become a part of our daily routine.
Advocacy, defined as the act or process of supporting a cause or proposal (Merriam Webster, n.d.), has transformed over time. Advocacy can range from raising awareness, to direct lobbying for change. The digital age has made it simple and efficient for individuals and organizations to instantly reach large audiences via the internet. The number of websites has grown exponentially, from an estimated 3,000 sites in 1994, to 1.88 billion in 2021 (Armstrong, 2021). This abundance of existing websites can be overwhelming, and it can be challenging to find the knowledge and sources you need to get started. The websites listed below are not all-inclusive but may be helpful in locating the knowledge or resources needed to be an advocate in healthcare.
American Association of Colleges of Nursing
AACN is a nonpartisan organization that serves to educate and advocate for nursing education, research, and practice. They host an annual Student Policy Summit and publish a Washington Weekly newsletter. The site has a “take action” section with letters you can send to your representatives.
American Association of Nurse Practitioners (AANP)
The AANP website contains links and resources for tracking the latest federal and state legislation pertaining to nurse practitioners and healthcare. The advocacy center lists several legislative issues with electronic letters of support that can be sent to representatives. Members can subscribe to receive e-bulletins, Smart Briefs, and Government Affairs Updates.
The ANA believes that advocacy is a pillar of nursing. The advocacy section of this website has the latest federal and state legislation and contains an advocacy toolkit with tips on becoming an effective nursing advocate. You can subscribe to their blog, Capital Beat.
Association of Women's Health, Obstetric and Neonatal Nurses
(AWHONN) is an organization dedicated to improving the health of women and newborns and strengthening the nursing profession. This website highlights the organization's key legislative priorities and phone scripts to use when calling your representatives regarding specific bills.
Congress.gov is the official website for U.S. federal legislative information. The site provides access to legislative information for Members of Congress, legislative agencies, and the public. Current and past legislation or topics can be queried and there are many resources along with a section to contact your state representative.
This website was created to make it easier for citizens and communities to understand the regulatory process and to participate in government decision- making. You can explore federal agencies and sub-agencies, such as the Centers for Disease Control (CDC), or topics of interest.
Health Affairs is a journal of health policy thought and research. They produce a blog called Health Affairs Forefront, have a series of podcasts, and publish Health Policy Briefs which examine issues currently being debated in health policy and research. These briefs provide a clear, comprehensive, and impartial overview.
March of Dimes is a well-known, well-established organization that supports research, programs, and education for families. They publish PeriStats and a State Grade report. Their advocacy efforts fall into 4 categories: Access to care, research and surveillance, prevention and education (including prematurity prevention), substance abuse, environmental health, and tax-exempt organization issues.
National Coalition for Infant Health (NCfIH)
The National Coalition for Infant Health educates and advocates on behalf of premature infants from birth to age two. (NCfIH) is a collaborative of professional, clinical, community health, and family support organizations that promote patient-centered care for premature infants and their families.
NANN is a part of this coalition, which is comprised of 63 national professional nursing associations dedicated to building consensus and advocating on a wide spectrum of healthcare issues, including practice, education, research, and regulation.
NOA connects elected and staff leaders of professional nursing organizations to collaborate and provide a forum for information exchange and the sharing of resources and best practices. NOA is a collaborative community convening leaders of professional nursing organizations to address common interests and achieve shared goals. NOA sponsors the annual Nurse in Washington Internship (NIWI) each year. NANN is a member of this alliance.
National Perinatal Association
The National Perinatal Association (NPA) is an interdisciplinary organization of professionals, parents, students, and advocates.
NANN is dedicated to advocating for NICU infants and their parents, as well as supporting our nursing profession. Additional resources can be found on the NANN website, including policy and advocacy toolkits. NANN’s current advocacy priorities are listed below with an example of websites that inform and advocate for each topic.
- Disparities Within Neonatal Care: March of Dimes
- COVID-19 Impact on Patients and Nurses: NANN
- Mental Health of NICU Families and Nurses: National Perinatal Association
- Nursing Workforce Development:
- Paid Family Leave: 1,000 Days
- Nutrition and Breastfeeding: U.S. Breastfeeding Committee
References:
Armstrong, M. (2021). How many websites are there? Statista.
https://www.statista.com/chart/19058/number-of-websites-online/
Merriam-Webster. (n.d.). Advocacy. In Merriam-Webster.com dictionary. Retrieved March 24, 2022, from https://www.merriam-webster.com/dictionary/advocacy
January 2022 - Addressing Racial Disparities in the NICU
Raymond K. Riley, BSN RNC-NIC C-NPT C-NNIC
With Black History Month around the corner, it is important to discuss and recognize disparities within the NICU. While it might not be talked about often enough, it is known that there are significant disparities in healthcare and health outcomes for BIPOC (black, indigenous, and people of color) patients in our country. Three contributors to health disparities have been described: increased risk for preterm birth, lower quality of care, and socioeconomic disadvantages. This remains true for our pregnant patient population and NICU population as well. In order to assess our delivery of care in the NICU, a composite indicator was developed in California called Baby-MONITOR. This can be used to measure the quality of care provided to very low birth weight (VLBW) infants based on 9 process and outcome measures of quality chosen by a panel of experts. This tool may be applied to any NICU to assess the quality of care delivered (Profit et al., 2014). In 2017, a retrospective analysis of 18,616 patients from 134 NICUs in California specifically from 2010 to 2014 was conducted using Baby-MONITOR. It was determined that there were clinically and statistically significant racial and/or ethnic variations in quality of care between NICUs and even within NICUs. There were also findings that indicated the significant quality disparities were within modifiable measures, including whether a VLBW patient received antenatal steroids or not (Profit et al., 2017). The disparities that are apparent in NICUs across the country can be addressed and, in some cases, have been shown to nearly disappear when robust efforts are made through individualized process engineering and culturally competent care. Looking ahead, we have discussed this, analyzed this, and studied this extensively, however; what are we going to do to bring about a change in these statistics?
One of the largest recent efforts to address the aforementioned disparities is the Black Maternal Health Momnibus Act of 2021 (H.R. 959). This bill, which has been mentioned time and time again, would build on efforts to extend postpartum Medicaid coverage to 12 months. It would also extend much further by investing in social determinants of health, funding community-based organizations to improve health outcomes, support patients with substance use disorder, and much more (H.R. 959, 2021). This bill is a consolidated effort by the Black Maternal Health Caucus to address health disparities. It provides a multifaceted approach to attacking the health disparities lamented by our broken system. This legislation has been introduced but has yet to be acted upon by Congress. Similarly, the Build Back Better Act (H.R. 5376) aims to enact many of the provisions from the Momnibus Act, allocating millions of dollars toward social determinants of health. There is also money allocated to strengthen the nursing workforce, including $500 million for the Nurse Corps and $170 million to grow and diversify the nursing workforce in maternal and perinatal health. Additionally, there are provisions to expand research and data collections to determine inequitable areas in our healthcare system (H.R. 5376, 2021). This bill has faced tremendous partisan struggles in Congress and has not moved forward. Many of these efforts are stalled because the legislation would also expand Medicaid coverage in the postpartum period nationally.
The expansion of Medicaid coverage is a tangible area that can be explored to improve care in the postpartum period. Under the Affordable Care Act, states are able to extend coverage for patients postpartum. For example, in Mississippi, the current program allows for 60 days of postpartum healthcare coverage. After that 60-day period, patients are cut off and lose health coverage. A Maternal Mortality Review Committee, which found that almost 40% of pregnancy-related deaths in the state occurred more than 6 weeks after giving birth, recommended extending coverage to a full year postpartum (Harris, 2022). This measure is still awaiting action by the state legislature. Previous proposals have been unsuccessful as legislators attempted to determine the extent to which the governor’s office can control the state Medicaid agency. This session, bipartisan bills have been filed in both the house and senate to extend Medicaid coverage and a voting deadline has been set for committees to address this (Harris, 2022). Efforts at the state level can be used to address health disparities by recognizing the gaps in healthcare and insurance coverage and seeking out solutions. Many states have made efforts to expand their Medicaid coverage, but 12 have yet to move forward with an extension. While there are many efforts on both sides of the aisle to address health disparities, we aren’t going to make any progress until we stop letting “the aisle” decide the quality of outcomes for our patients.
NANN strongly believes that all infants, regardless of race, parental economic or educational status, or geographic area should receive equitable, quality healthcare. As nurses, we have to advocate for our patients and their families to the fullest extent. There are several ways to get involved:
- Learn and stay abreast of the issues.
- Engage with your local community leaders and stakeholders.
- Share what you learn and contact your House or Senate representatives about the importance of reducing disparities.
- Advocare for awareness and support for the issues through your professional organizations.
We can do our part to help address health disparities, and demand change through action on a public policy level. Every parent and infant deserves to receive the best care possible.
References:
Black Maternal Health Momnibus Act of 2021, H.R. 959, 117th Cong. (2021). https://www.congress.gov/bill/117th-congress/house-bill/959.
Build Back Better Act, H.R.5376, 117 Cong. (2021) https://www.congress.gov/bill/117th-congress/house-bill/5376
Harris, B. (2022, January 16). As Mississippi fights for abortion ban, doctors push to expand Medicaid for new moms. NBCNews.com. Retrieved from https://www.nbcnews.com/news/us-news/mississippi-medicaid-infant-maternal-mortality-rcna12249
Profit, J., Gould, J. B., Bennett, M., Goldstein, B. A., Draper, D., Phibbs, C. S., & Lee, H. C. (2017). Racial/Ethnic Disparity in NICU Quality of Care Delivery. Pediatrics, 140(3), e20170918. https://doi.org/10.1542/peds.2017-0918
Profit, J., Kowalkowski, M. A., Zupancic, J. A., Pietz, K., Richardson, P., Draper, D., Hysong, S. J., Thomas, E. J., Petersen, L. A., & Gould, J. B. (2014). Baby-MONITOR: a composite indicator of NICU quality. Pediatrics, 134(1), 74–82. https://doi.org/10.1542/peds.2013-3552
December 2021 - The Impact and Importance of Vaccination for Pregnant Mothers
Susie Taylor, BSN RNC-NIC
From stay-at-home orders to virtual doctor’s appointments, to mask mandates, to giving birth alone, COVID 19 has shifted the care patients receive across the spectrum of healthcare. Now, on the cusp of 2022, we have a vaccine that helps prevent the spread of the disease and lessen its impact if contracted. The U.S. and the world have experienced a slow and sometimes fleeting “return to normalcy.” That said, the impact COVID 19 has had on healthcare is undeniable, as are the unforeseen outcomes that are continuing to unfold especially for pregnant women.
Many of the outcomes impacting pregnant women can be offset with vaccination before or during pregnancy.
To address negative outcomes of all sorts, NANN is clear in its mission: “Through the leadership of NANN's Health Policy and Advocacy Committee, NANN seeks to optimize care and health outcomes for neonates and their families.” The challenges created by the virus are testing our abilities to optimize care and health outcomes. In the United States 61.4 % of the population is fully vaccinated against COVID 19 (Our World Data, 2021). Portions of the remaining 38.6% of unvaccinated people are pregnant or lactating women. In the face of various beliefs on vaccinations and the deadliness of COVID 19 we know this: Pregnancy is a severe risk factor for the disease. Contracting COVID 19 while pregnant makes you more likely to be admitted to the ICU, require mechanical ventilation, extracorporeal membrane oxygenation, and an obvious worst case is maternal and infant death (CDC, 2021). If that is not startling enough there is new evidence suggesting that contracting COVID 19 while pregnant leads to additional adverse outcomes such as an increased risk for preeclampsia, preterm birth, and still birth (Jamieson & Rasmussen, 2021). Vaccination can help prevent contracting the disease and allow for a milder course if infected to avoid these tragic complications.
The impact of COVID 19 on mental health has become a national crisis, and the same is true for antenatal and postpartum populations. Fears surrounding contracting COVID 19 and passing it on to a child are real and prevalent. While it looks that there is minimal risk from vertical infection during pregnancy there is limited but promising research that the vaccine does provide antibodies and some protection to the infant after delivery (ACOG, 2021). Another harmful, but down-played factor is the isolation COVID 19 causes. Mothers who have COVID 19 are often fearful they will pass it on to their child after they deliver. They are at times isolated from their child and separated from other loved ones and persons of support. The lack of contact with their child can impact bonding, milk production, and increase the risk of postpartum depression and anxiety. Guilt associated with passing the virus to an infant postpartum, or the fear of the infant getting sick, can also negatively impact mothers’ mental health and the family unit. Vaccination is key in preventing this. While vaccines are imperfect and breakthrough cases do happen, especially when new variants such as Omnicron emerge, there is peace of mind knowing that a parent has done everything possible to decrease the risk of contraction for their child. Let us not overlook the value of that peace of mind.
The United States has been striving for improved social programming to improve the maternal and infant mortality statistics within the U.S. These efforts and outcomes of such programming are undermined by the lack of vaccination causing widening gaps of access to care. The impact of large numbers of unvaccinated people threatens our ability to deliver healthcare in a timely and efficient manner. The longer the pandemic continues due to large number of unvaccinated people, social programs will not meet their potential including advances in maternal and infant mortality.
As nurses we must continue to provide our patients and families the best care, which includes educating them on the positive impact vaccination can have on antenatal and postpartum populations. This education should not just focus on the generic health benefits, but it needs to include mental health considerations and societal implications as well.
References:
CDC.gov, 2021. “Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States” Dec. 17, 2021. https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html#pregnant
Goncu Ayhan, S., Oluklu, D., Atalay, A., Menekse Beser, D., Tanacan, A., Moraloglu Tekin, O., & Sahin, D. (2021). COVID-19 vaccine acceptance in pregnant women. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics, 154(2), 291–296. https://doi.org/10.1002/ijgo.13713
Jamieson, D. J., & Rasmussen, S. A. (2021). An update on COVID-19 and pregnancy. American journal of obstetrics and gynecology, S0002-9378(21)00991-1. Advance online publication. https://doi.org/10.1016/j.ajog.2021.08.054
Our World in Data, 2021. https://ourworldindata.org/covid-vaccinations?country=USA accessed December 18, 2021.
The American College of Obstetrician and Gynocologists, 2021. “COVID-19 and Pregnancy: Conversation Guide” December 2021. https://www.acog.org/covid-19/covid-19-vaccines-and-pregnancy-conversation-guide-for-clinicians
November 2021 - Nursing Priorities within the Build Back Better Act
Tommie Farrell, BSN RNC
In the last two weeks, Congress has passed into law the Infrastructure Investment and Jobs Act (H.R.3684), and the House recently passed the Build Back Better Act (H.R. 5376). While the Build Back Better bill will go to the Senate, (and likely will see significant changes from its current provisions), it is a big step that the House passed this bill. We, as healthcare professionals, should care about and understand what is happening with this legislation.
It may appear on the surface that the infrastructure bill would have little correlation to healthcare however, we know as nurses that access to state-of-the-art infrastructure, including transportation, water systems, broadband, and power grids will empower Americans to attain both preventive healthcare, and care for their healthcare needs. These investments will help rural areas have access to telemedicine and other services, improve access to running and/or safe drinking water for those who have no access to either, and will improve roads and bridges making it possible for rural healthcare providers to get to outlying communities that currently have no access. The inadequate conditions this bill addresses ultimately trickles down to our families and our small most vulnerable patient population.
The Build Back Better Act (H.R. 5376) includes priorities that address nursing education and practice, and these essential resources are integral as we support the public health of our nation and our current and future nursing workforce. NANN and NANNP alongside the Nursing Community Coalition (NCC) are proud to see the following provisions incorporated in the House-passed bill including:
- Support for Nursing Education Pathways: $500 million for nursing education enhancement and modernization grants to support the needs of nursing students, help retain and hire diverse faculty, modernize nursing education infrastructure, and create and expand clinical education.
- Investments for Nurses and Advance Practice Registered Nurses (APRNs) working in Underserved Areas: $500 million for the Nurse Corps to support scholarships and loan repayment for nurses and APRNs who work in areas that need them the most.
- Includes Major Provisions from the Momnibus Act, such as: $170 million to grow and diversify the nursing workforce in maternal and perinatal health; $100 million in Maternal Mental Health Equity grant programs; $85 million in funding for education and training at health professions schools to identify and address health risks associated with climate changes, including for pregnant, lactating, postpartum or individuals who are looking to become pregnant; $50 million in funding for antidiscrimination and bias training; and millions for other programs including promoting equity in maternal health outcomes through digital tools. Furthermore, the bill includes resources to support public health and public health infrastructure, grants for mental health programs and pandemic preparedness initiatives, as well as other provisions that aim to create a more equitable health care system.
NANN, NANNP, and our NCC partners look forward to working with the Senate and urge them to include these provisions in their version of the Build Back Better Act. We remain deeply committed to advancing these priorities that support our nursing students, nurses, APRNs, and the patients they serve.
The Build Back Better bill is more about "human infrastructure" which is easier to relate back to neonatal nursing. We can see a direct line between the priorities listed above and improved health outcomes for our littlest and most vulnerable babies and their families. This legislation touches on multiple aspects of ensuring a healthy nation, especially in its provisions for families and children. It provides for permanent Children's Health Insurance Programs (CHIP). It will require Medicaid and CHIP to provide 12 months of Postpartum care with Medicaid benefits, which is a great benefit for underserved families. It also helps us to identify who among these new mothers is experiencing Postpartum depression because they will be in a program that ensures that healthcare providers will see them in this postpartum period. Other provisions and funds are being provided to address Public Health Infrastructure, Behavioral Health, Paid Leave, lowering Drug Costs, Diversity, Inclusion, Perinatal, Neonatal enhancement of Diverse Nursing workforce are also addressed. This legislation increases our ability to lift our families and patients into health care inclusion.
If you look at the content, it is designed to improve lives and narrow the gap in healthcare. While it is impossible to talk about all of the details here, I encourage you to think about it, engage in learning more and realize that we, as a Nursing workforce, will be a part of it. (and need to be a part of it). This is an opportunity for us to demonstrate how important this legislation is for our patients with our experience. I encourage you to contact your elected officials in the United States Senate and encourage them to keep the above listed nursing priorities in the Build Back Better Act, and to thank your elected officials in the House of Representatives for passing this legislation.
References:
American Hospital Association. House Passes Build Back Better Act with Significant Health Care Provisions. Accessed November 22, 2021. https://www.aha.org/special-bulletin/2021-11-18-house-passes-build-back-better-act-significant-health-care-provisions
Build Back Better Act, H.R.5376, 117 Cong. (2021) https://www.congress.gov/bill/117th-congress/house-bill/5376
Infrastructure Investment and Jobs Act, H.R.3684, 117 Cong. (2021) https://www.congress.gov/bill/117th-congress/house-bill/3684
NCC Statement on the House Passage of the Build Back Better Act. Accessed November 22, 2021. https://131a058d-9186-c34a-b6f8-7f4cb1fce3f0.filesusr.com/ugd/148923_1d75bcdd0fb041a694f6dbc29c237a05.pdf
October 2021 - The Opioid Epidemic and the Maternal Mortality Crisis
Raymond K. Riley, BSN RNC-NIC C-NPT C-NNIC
The opioid epidemic in the United States has had devastating effects across the lives of people affected and throughout the healthcare continuum. People suffering from opioid addiction are diagnosed with opioid use disorder (OUD). OUD is defined as a problematic pattern of opioid use resulting in symptoms such as tolerance, withdrawal, craving, or an inability to cut down or control opioid use. This disease does not discriminate and can be seen in a significant population of our pregnant people. There are risks associated with withdrawal or detox from opioids during pregnancy, so it is currently not recommended. This leaves pregnant people with limited options to safely treat OUD. The current standard is medication-assisted treatment (MAT) with a drug like methadone. MAT during pregnancy minimizes opioid withdrawal, reduces risk-taking behavior, and decreases the chance of exposure to and infection with Hepatitis C and HIV, which in turn, decreases the chance of transmission of these infectious diseases to the infant. This treatment plan, while a much better option than unregulated, illicit drug use, still poses a risk for the developing infant. Infants exposed to MAT medications will exhibit some level of withdrawal and likely be diagnosed and treated for neonatal abstinence syndrome (NAS) (Krans & Patrick, 2016). It is very important that we as healthcare providers recognize that infants diagnosed with NAS and parents diagnosed with OUD are people first and should be treated with the same compassionate care provided to all other patients and parents.
As the epidemic continues to smolder away, we are also facing a maternal mortality crisis that is directly linked to the epidemic. Maternal mortality is defined as death occurring during or within one year after pregnancy, caused by pregnancy or childbirth complications, including suicide, overdose, or other death resulting from a mental health or substance use disorder attributed to or aggravated by pregnancy or childbirth complications (H.R. 959, 2021). The maternal mortality rate in the United States has trended upward in recent years. In fact, the United States ranks highest for maternal mortality out of the Organization for Economic Co-Operation and Development (OCED) nations. Specifically, the overall maternal mortality rate in the US was 20.1 per 100,000 live births in 2019. This rate was more than double (44.0 per 100,000 live births) for non-Hispanic black persons. States are actively working to address these obvious inequities in our system and combat a high mortality rate by using Maternal Mortality Review Committees (MMRCs). MMRCs are used to perform comprehensive reviews of pregnancy-related deaths and put forth recommendations to prevent them. Many MMRCs have concluded that much more emphasis needs to be placed on preventing and treating OUD. The current COVID-19 pandemic and declining mental health have contributed to the continued prevalence of OUD in a wide spectrum of patient populations as well (Platt & Hanlon, 2021). A barrier to combating these issues in our pregnant patient population is inadequate healthcare coverage. More than 40% of births in the US are covered by Medicaid, and it can be difficult to get adequate coverage and reimbursement of mental health and OUD treatment during pregnancy. The MMRCs commonly recommend that states provide adequate insurance coverage for multifaceted screenings, conduct system and medical record reviews to monitor risk factors and patterns, and perform universal screenings of pregnant individuals (Platt & Hanlon, 2021). These steps would help to improve early diagnosis of OUD and other conditions early in pregnancy or even before it.
In Congress, there is currently sweeping legislation to address these health disparities and even specifically the effects of the opioid epidemic on our pregnant population. The Black Maternal Health Momnibus Act of 2021 (H.R. 959), introduced by Representative Underwood (D-IL-14), is comprised of 12 bills that work in tandem to ensure there is equitable access to healthcare at all stages of pregnancy. This widespread approach aims to increase grant funding, enhance data collection, and improve public health programs. To address OUD in pregnancy, this act offers grants to programs and resources in the community that provide evidence-based treatments for OUD in black pregnant and postpartum individuals. This also establishes a task force, with one of the responsibilities detailed as reviewing frequency and causes of OUD. In addition, there is a push to raise awareness and reduce stigma behind OUD with specific focus on pregnant and postpartum individuals of minority backgrounds (H.R. 959, 2021). In summation, this act intends to provide significant grant funding to expand access to treatment, collect data, raise awareness, reduce stigma, and take better care of our pregnant and postpartum minority population to reduce inequities in our healthcare system. The act is currently being reviewed in congressional committees and has yet to receive a vote.
As NICU nurses and APRNS, we are at the frontlines of taking care of infants and their parents. Change can start with us by reducing the stigma and ensuring that our patients suffering from NAS and their parent(s) with OUD are treated equally with respect and care. They should be encouraged to bond and take care of their baby as much as any other parent. We have the power to change the culture, leave judgement at the door, and make a significant, positive impact on their lives, which is needed now more than ever.
References:
Black Maternal Health Momnibus Act of 2021, H.R. 959, 117th Cong. (2021). https://www.congress.gov/bill/117th-congress/house-bill/959.
Krans, E. E., & Patrick, S. W. (2016). Opioid Use Disorder in Pregnancy: Health Policy and Practice in the Midst of an Epidemic. Obstetrics and gynecology, 128(1), 4–10. https://doi.org/10.1097/AOG.0000000000001446.
Platt, T., & Hanlon, C. (2021). State Maternal Mortality Review Committees Address Substance Use Disorder and Mental Health to Improve Maternal Health. National Academy for State Health Policy. Retrieved from https://www.nashp.org/wp-content/uploads/2021/08/maternal-mortality-review-committees-address-substance-use-disorder-and-mental-health.pdf
September 2021 - October is Maternal Mental Health Month
Julie Sundermeier, DNP APRN-NP NNP-BC
Maternal mental health (MMH) conditions are the most common complications of pregnancy and childbirth, affecting as many as 1 in 5 women, and 3 in 5 women of color each year in the United States. MMH conditions include depression, anxiety disorders, obsessive compulsive disorder, post-traumatic stress disorder, bipolar illness, and substance use disorders. (CDC). Screening to detect, refer, and treat MMH lacks a consistent and standardized approach, and needed services may not be timely or readily available.
Additionally, when compared to mothers of term infants, mothers of preterm infants hospitalized in the NICU experience disproportionally elevated rates of post-partum psychological distress. As NICU nurses, we witness the stress that mothers experience on a daily basis. NICU parents experience loss of the parenting role and disruptions to parent-infant bonding. (Green, et al., 2015; Lean, Rogers, Paul, Gerstein, 2018; Ouyang, et al, 2020). The intensive care environment and the critical condition of their newborn can be overwhelming and traumatic. In addition, MMH issues can have adverse effects on infant and child well-being with associated effects on cognitive, behavioral and emotional development. Additional impacts of mental health on maternal-infant health were summarized in a recent historical perspective article by Ouyang et al. (2020).
In an effort to create a national strategy for MMH the TRIUMPH Act (The Taskforce Recommending Improvements for Unaddressed Mental Perinatal and Postpartum Health) for New Moms Act of 2021 was recently introduced in both the House and Senate. This bipartisan legislation was introduced in the House (H.R. 4217) by Nanette Barragán (D-CA), Larry Buschon (R-IN), Young Kim (R-CA), and Lisa Blunt Rochester (D-DE) and in the Senate (S. 2779) by Thom Tillis (R-NC) and Maggie Hassan (D-NH). The TRIUMPH Act calls for the formation of a maternal mental health task force of federal agencies. This task force would review and identify existing programs and best practices addressing maternal mental health conditions. H.R. 4217 outlines the following proposed actions:
- increasing prevention, screening, diagnosis, intervention, treatment, and access to care, including clinical and nonclinical care such as peer-support and community health workers, through the public and private sectors;
- providing support for pregnant or postpartum individuals who are at risk for or experiencing a maternal mental health condition, and their families as appropriate;
- reducing racial, ethnic, geographic, and other health disparities for prevention, diagnosis, intervention, treatment, and access to care;
- identifying opportunities for local and State-level partnerships;
- identifying options for modifying, strengthening, and coordinating Federal program and activities
- providing recommendations to ensure research, services, supports, and prevention activities are not unnecessarily duplicative; and
- planning, data sharing, and communication within and across Federal departments, agencies, offices, and programs
Mental Health for NICU families is one of NANN’s advocacy priorities. Legislation such as the TRIUMPH bill could further the recognition and support for maternal mental health. Please contact your states Congressional representatives and ask them to support this important legislation.
References:
CDC. Depression among women. https://www.cdc.gov/reproductivehealth/depression/index.htm. Accessed September 24, 2021.
Green, M. M., Rossman, B., Patra, K., Kratovil, A. L., Janes, J. E., & Meier, P. P. (2015). Depressive, anxious and perinatal post-traumatic distress in mothers of very low birth weight infants in the NICU. Journal of Developmental and Behavioral Pediatrics; 36(5): 362-370. doi:10.1097/DBP.0000000000000174.
H.R.4217- 117th Congress (2021-2022): Triumph for New Moms Act 2021. (2021, June 29). https://www.congress.gov/bill/117th-congress/house-bill/4217
Lean, R. E., Rogers, C. E., Paul, R. A., & Gerstein, E. D. (2018). NICU hospitalization: long-term implications on parenting and child behaviors. Current treatment options in pediatrics, 4(1), 49-69. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5986282/
Ouyang, J. X., Mayer, J. L. W., Battle, C. L., Chambers, J. E., & Salih, A. N. I. (2020). Historical perspectives: Unsilencing suffering: Promoting maternal mental health in neonatal intensive care units. NeoReviews; 21(11) e708-e715. DOI: 10.1542/neo.21-11-e708
S.2779- 117th Congress (2021-2022); A bill to amends the Public Health Service Act to provide for the establishment of a Task Force on Maternal Mental Health, and for other purposes. (2021, September 21). https://www.congress.gov/bill/117th-congress/senate-bill/2779
August 2021 - Health Disparity in the United States
Julie E. Williams, DNP CRNP NNP-BC
Health disparity, sometimes referred to as health inequalities or health inequities, has many definitions. According to the Center for Disease Control and Prevention (CDC, 2011), health disparity is defined as "differences in health outcomes and their determinants between segments of the population, as defined by social, demographic, environmental, and geographic attributes." Healthy People 2020 defined health disparity as "a particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage". Health disparities affect disadvantaged populations and impose a disproportionate burden of morbidity and mortality based on socioeconomic status, race/ethnicity, or gender. Affected populations often include people of color, the lesbian, gay, bisexual, transgender, queer (LGBTQ), disabled, and the poor. Contributing factors include lack of access to health care, education, income, nutrition, lifestyle, and environment.
Rooted in deeper social, political, and historical context, race and ethnicity have been the most persistent health disparity. Through the development of local, state, and federal laws and policies, the government has helped shape the direction of America's discrimination. For example, initiatives like zoning laws compounded with low pay prevented African Americans from owning homes in certain areas. Meanwhile, other zoning laws designated areas adjacent to predominantly African American neighborhoods for industry, contributing to lower property values.
In 2018, non-Hispanic Black women experienced an infant mortality rate greater than two times that of non-Hispanic white women, Non-Hispanic Asian women, and Hispanic women (Ely & Driscoll, 2020). Compared with other races, non-Hispanic Black women also had the highest neonatal mortality rate of 7.06 infant deaths per 1,000 live births (Ely & Driscoll, 2020). Finally, infant deaths related to prematurity, low birth weight, maternal complications, and SIDS were highest among non-Hispanic Black women.
The last 50 years have brought forth several efforts to facilitate the reduction of health inequities. The CDC's Health Disparity and Inequalities Report of 2011 and 2013 provided an analysis of the trends and variations in health disparities and inequalities for deaths and illness, use of health care, behavioral risk factors for disease, chronic diseases, environmental hazards, and social determinants of health at the national level, among others. It is essential to understand that efforts to reduce health disparities must be multidimensional. Federal initiatives and action plans like Healthy People 2020 and the Health and Human Services Action Plan to Reduce Racial and Ethnic Health Disparities can also provide direction to improve the racial and ethnic gaps. Local programs should be focused on the community and facilitate the equitable allocation of resources.
In 2020, NANN endorsed healthcare equality for all infants irrespective of race, parental economic or educational status, or geographic area in a position statement on Racial Disparity in the NICU (NANN, 2020). Recommendations included small steps that could be taken by all NICU providers including examining your own personal biases, inviting parental diversity in unit committees, and having open discussions about racial disparities. All neonatal nurses have a responsibility to help create health equity.
References:
CDC's Health Disparities and Inequalities Report, 2011 (2011). Association of Schools of Public Health.
Ely, D. M. & Driscoll, A. K. (2020). Infant mortality in the United States, 2018: Data from the period linked birth/infant death file. National Vital Statistics Report, 69(7), 1-18. https://www.cdc.gov/nchs/data/nvsr/nvsr69/NVSR-69-7-508.pdf
HHS action plan to reduce racial and ethnic health disparities (2011). Department of Health & Human Services, USA.
Racial Disparity in the NICU, (2020, June) National Association of Neonatal Nurses. http://nann.org/uploads/About/PositionPDFS/Racial_Dispariy_in_the_NICU_-_FINAL_6.12.20.pdf
Meyer, P. A., Yoon, P. W., & Kaufmann, R. B. (2013). Introduction: CDC Health Disparities and Inequalities Report - United States, 2013. Morbidity and Mortality Weekly Report. Supplement, 62(3), 3-5. https://www.ncbi.nlm.nih.gov/pubmed/24264483
Office of Disease Prevention and Health Promotion. (n.d.). Healthy people 2020. Healthy People 2020. https://www.healthypeople.gov/2020/.
Sciences, N. A. of, Engineering, & Medicine, and. (2017, January 11). Native American Health: Historical and legal context. Communities in Action: Pathways to Health Equity. https://www.ncbi.nlm.nih.gov/books/NBK425854/.
July 2021 - Advancing FASD Research, Services, and Prevention
Raymond Riley, BSN RNC-NIC C-NPT
Fetal Alcohol Spectrum Disorder (FASD) is an often misunderstood and under-diagnosed disorder. When a fetus is exposed to alcohol, a known teratogen, a lifetime of harm can be brought upon the infant and affect the individual as they develop through life. Fetal alcohol syndrome is characterized by dysmorphic facial features, abnormalities in brain structure, neurological deficits, and sensory and neuropsychological abnormalities (Wozniak et al., 2019). In the case of FASD, the facial features may not be present. However, a person with FASD can still suffer from many of the same neuropsychological issues as the individual with Fetal Alcohol Syndrome (FAS).
A correct diagnosis poses a challenge due to a lack of accurate reporting of maternal alcohol use, specific biomarkers for testing, and the wide variety of physical symptoms that may or may not present. There is a high prevalence of FASD worldwide due to the widespread use of alcohol, including during pregnancy. It is vital that alcohol use during pregnancy be identified early to allow for early intervention, proper diagnosis, and better outcomes for the exposed infant (Wozniak et al., 2019). Less severe cases of FASD are even more difficult to diagnose and often slip through the cracks. The reluctance to admit alcohol use in pregnancy plays a large role in this issue as well (American Bar Association, 2018). There is currently important work being done in the U.S. Congress to address this disparity in identification, research, and intervention.
The FASD Respect Act (H.R. 4151 & S. 2238), a bipartisan effort, has already been introduced to Congress. It is co-sponsored by Representative Betty McCollum (D-MN) and Representative Don Young (R-AK) and Senator Lisa Murkowski (R-AK) and Senator Amy Klobuchar (D-MN) in the House and Senate respectively. This legislation allocates $118 million to screenings, research, identification, and more informed services at the local, state, and federal level in addition to the private sector. Even more importantly, this bill establishes a clearer and stronger societal commitment to advancing research and ensuring that persons with FASD and their caregivers have access to essential services. This bill will also replace defunct and outdated organizations with a National Advisory Council on FASD and establish a Center for Excellence focused on FASD to be the go-to entity when developing or improving best practices for FASD prevention, diagnosis, and intervention (National Organization on Fetal Alcohol Syndrome, 2021). Adults with FASD can exhibit behavioral and psychological disturbances leading to more socioeconomic problems for these individuals and their caregivers (Wozniak et al., 2019). The American Bar Association (ABA) has acknowledged this and addressed it through resolutions to protect these individuals.
The resolution passed by the ABA urges attorneys and judges at all levels to be aware of FASD and respond effectively to juveniles and adults in the criminal justice system. Rather than overlooking how FASD can be a contributing factor, this resolution stresses the value of collaborating with medical, mental health, and disability experts to properly address the needs of these individuals. As a whole, this initiative strives to improve the civil, juvenile, and criminal legal representation for individuals with FASD (American Bar Association, 2018).
As NICU nurses, we are also on the front line of identifying potential cases of FASD. We should strive to provide these infants with all the resources that they and their caregivers will need to encourage the best possible outcome in the long term. The FASD Respect Act goes hand in hand with this mission to optimize our ability as healthcare workers to identify and treat.
As we approach FASD Awareness Month (September) and this important legislation moves through Congress, it is imperative that NICU nurses advocate for the FASD Respect Act on behalf of our patients and their families. Reach out to your local representatives and senators to ask for their support. To identify your representatives and senators, visit www.usa.gov/elected-officials.
References:
American Bar Association. (2018). FASD Resolution. https://www.americanbar.org/groups/public_interest/child_law/resources/attorneys/fasd-resolution/.
National Organization on Fetal Alcohol Syndrome. (2021). The FASD Respect Act. NOFAS Policy And Training Center. https://nofaspolicycenter.org/the-fasd-respect-act/.
Wozniak, J.R. Riley, E. P. Charness, M.E. (2019). Clinical presentation, diagnosis, and management of fetal alcohol spectrum disorder. Lancet Neurol., 18 (8) (2019), pp. 760-770, 10.1016/S1474-4422(19)30150-4.
June 2021 - Momnibus Act Seeks to Improve Maternal Health Outcomes, Reduce Disparities
Julie Sundermeier, DNP APRN-NP NNP-BC
The United States has the highest maternal mortality rate of any high-resource country, and the rate continues to rise. 700 women die in the U.S. every year due to pregnancy or delivery complications, and women of color have even higher mortality rates. Black women are three to four times more likely to die from a pregnancy-related cause than White women, and Native American and Alaskan Native mothers have a 2.5-fold risk. (Petersen et al., 2019). This disparity can be attributed to factors such as variations in healthcare, underlying chronic conditions, structural racism, and implicit bias.
The Black Maternal Health Momnibus Act of 2021 (H.R. 959) was introduced on February 28, 2021, to help end preventable maternal mortality and morbidity for all women, and to reduce disparities in maternal health outcomes. The Momnibus Act is composed of 12 individual bills that were each sponsored by a member of the House Black Maternal Health Caucus to build on existing legislation to address the maternal health crisis for all women, especially those of color. Also addressed are actions to mitigate adverse maternal health outcomes associated with climate change and to improve maternal vaccination rates.
Bill summary:
The Black Maternal Health Momnibus Act will:
- Address social determinants of health with a focus on areas with high rates of maternal mortality and severe morbidity with disparate outcomes.
- Award grants to community-based organizations to improve maternal health outcomes for underserved populations. Provide training in racial bias and discrimination to healthcare providers in maternity settings.
- Implement a maternity care coordination program for veterans with community maternity care providers that have training and support concerning the unique needs of pregnant and postpartum veterans, particularly regarding service-related mental and behavioral health conditions.
- Improve diversity in the perinatal workforce to allow for culturally congruent maternity care for mothers of color.
- Improve data collection processes and quality measures to better understand the causes of the maternal health crisis in the United States.
- Develop support systems for mothers with maternal mental health conditions and substance use disorders.
- Improve maternal health care and support for incarcerated moms.
- Invest in digital tools like telehealth to improve maternal health outcomes in underserved areas.
- Establish the Perinatal Care Alternative Payment Model Demonstration Project to allow states to test payment models for maternity care, including postpartum care, under Medicaid and the Children's Health Insurance Program (CHIP).
- Provide education and guidance for maternity care with COVID-19 and in future public health emergencies.
- Address health risks associated with climate change and environmental toxins, especially for members of racial and ethnic minority groups, pregnant or postpartum individuals, and children younger than age three.
- Raise awareness and increase rates of maternal vaccinations, especially in areas with high rates of unvaccinated individuals.
To change the racial inequalities in maternal-child health outcomes there needs to be action on a public policy level. The Momnibus Act has been endorsed by over 240 organizations. There are several ways to get involved:
- Spread the word on social media sites.
- Engage with local community leaders and stakeholders to garner support.
- Contact your representative in the House or Senate to tell them the importance of this issue.
- Advocate for awareness and support for the Momnibus Act through your professional organizations.
- Staying informed about Momnibus updates by following the U.S. House of Representatives Black Maternal Health Caucus on Twitter or their website.
References:
About the Caucus: Momnibus. US House of Representatives Black Maternal Health Caucus. (2020, February 3). https://blackmaternalhealthcaucus-underwood.house.gov/about.
Petersen, E. E., Davis, N. L., Goodman, D., Cox, S., Syverson, C., Seed, K., Shapiro-Mendoza, C., Callaghan, W. M., & Barfield, W. (2019). Racial/Ethnic disparities in pregnancy-related deaths- United States, 2007-2016. MMWR Morbidity and Mortality Weekly Report, 68(35);762–765. DOI: https://www.cdc.gov/mmwr/volumes/68/wr/mm6835a3.htm?s_cid=mm6835a3_w
May 2021 - Title VIII: What Does It Mean to Us as Nurses?
Michelle Cherry, DNP RN
This year, I was fortunate to represent NANN at the “Nurse in Washington Internship” (NIWI), offered through the Nursing Organizations Alliance (NOA). This program is designed to teach nurses how to advocate for themselves, their profession, and their patients, using our collective voices to improve and further the nursing profession, and healthcare. NIWI provides a forum for government and healthcare policy experts to speak to the nursing community about how each of us can utilize our voice to influence change. In addition, the internship sets up meetings to speak to our members of Congress and their healthcare aide in our home states. Even though this year NIWI had to be conducted virtually, we were still able to speak to other nurses within our state in depth about the issues that were most important to them so we could come together with a collective voice when we spoke to our members of Congress. From my state, we had pediatric, OR, obstetric, and geriatric nurses, as well as nursing instructors who came together to discuss topics that each felt required change in order to improve the care and livelihood of our patients.
A topic at this year’s NIWI was Title VIII, the Nursing Workforce Development program. Title VIII dates back to the 1964 Nurse Training Act, under President Lyndon Johnson, which was enacted in response to a significant nursing shortage, with more than 20% of hospital nursing positions vacant. The funds from this program were utilized to support nursing education, particularly to educate nurses who worked in rural or underserved areas. In addition, the funds provided loan forgiveness for clinical nurses and nursing educators in order to increase retention within the field.
Title VIII funds are awarded from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA). Advanced nursing education grants have helped educate nurse practitioners, clinical nurse specialists, nurse midwives, nurse anesthetists, nurse administrators, and public health nurses in primary care, unserved and rural areas.
For the last 57 years, Title VIII funding has helped supply the nursing workforce with qualified nurses. The Cares Act (H.R. 748-3) was signed into law on March 27, 2020 and included Title VIII nursing workforce funding under part IV of the healthcare provisions of the law. Title VIII would provide $137,837,000 per year from 2021 through 2025. The funding of this program is imperative in order to help address the undersupply of prepared nurses, as well as the looming loss of experienced nurses every year as our baby boomers retire.
According to the American Organization on Nursing Leadership, “in just a few short years there will be a shortage of almost one million nurses in America” (Title VIII Reauthorization, n.d.). More nurses are needed to care for our aging baby-boomers, to provide increased preventative care and to address chronic conditions. Currently, nursing schools are turning away qualified applicants due to lack of faculty, clinical sites, classroom space, clinical instructors, and budget limitations according to the American Association of Colleges of Nursing. In 2019 alone, nursing schools were forced to turn away 80,407 qualified applicants to nursing programs (Nursing Shortage, 2020).
As nurses, we need to continue to speak to our United States senators and representatives about the importance of these Title VIII funds. As for now, the spending bill will temporarily help support the needed growth of our nursing workforce.
References:
Key Provisions in the CARES Act for Health Care Providers. The National Law Review. (2020, March 30). https://www.natlawreview.com/article/key-provisions-cares-act-health-care-providers.
Nursing Shortage. American Association of Colleges of Nursing: The Voice of Academic Nursing. (2020, September). https://www.aacnnursing.org/News-Information/Fact-Sheets/Nursing-Shortage.
Stone, A. (2020, April 9). Title VIII Nursing Workforce Funding Included in CARES Act. ONS Voice. https://voice.ons.org/advocacy/title-viii-nursing-workforce-funding-included-in-cares-act.
Text - H.R.748 - 116th Congress (2019-2020): CARES Act. Congress.gov. (2020, March 27). https://www.congress.gov/bill/116th-congress/house-bill/748/text?s=2&r=26&overview=open#content.
Title VIII Reauthorization. American Organization of Nursing Leadership. (n.d.). https://www.aonl.org/advocacy/key-issues/title-viii-reauthorization.
April 2021 - Prenatal Care in a Pandemic
Raymond Riley, BSN RNC-NIC C-NPT
The COVID-19 pandemic has had widespread effects on nearly every facet of life in the United States. Many have not realized the profound impact the pandemic has had on antenatal care and the challenges posed for pregnant people and perinatal care teams.
During pregnancy, there is a litany of tests and screenings recommended to ensure a healthy fetus is growing and developing properly and that the pregnant person is also maintaining optimal health. Pre COVID-19 pandemic, the World Health Organization (WHO) recommended that antenatal care models include at least eight contacts to reduce perinatal mortality and ensure a positive pregnancy experience (World Health Organization, 2016). With the multiple surges of COVID-19 cases throughout the country, in-person prenatal appointments have become limited and restricted in nature. Often, the pregnant person has not been permitted to have support persons with them at appointments, meaning ultrasounds can become a solo affair. Other appointments have been pushed online, removing the personal experience from the prenatal care continuum.
When interviewed, Tali Bogler, a family doctor and low-risk obstetrics provider, described the challenges for pregnant people during the pandemic. Dr. Bogler reported that while the number of antenatal appointments has not necessarily decreased, the quality of appointments has in some cases. Pregnant people are saying appointments can feel rushed and less meaningful, especially virtually, as providers strive for efficiency and adjust to the virtual format. Some individuals have even been asked to do their own measurements at home, prompting the question: Are we missing anything (Brewster, 2020)? It is natural for a NICU nurse to wonder if the virtual, less personal antenatal care will lead to more NICU admissions down the road.
A major consequence of the COVID-19 pandemic described by pregnant people is the isolation felt during their few in-person appointments. Ultrasounds, which can't be done virtually, continue to be in-person. Due to the pandemic, ultrasound examinations are being somewhat limited, no longer used electively, and saved for when a risk is present or further diagnostic testing is needed (ACOG, 2021). When appointments are done in person, the change to not allow support persons in the room can increase anxiety when sometimes worrisome diagnostic tests are done and the results are communicated without the support of a loved one at the pregnant patient's side (Brewster, 2020). This change in antenatal care puts more emphasis on the nurses' role of supporting pregnant people and providing family-centered care.
For the time being, the American College of Obstetrics and Gynecology (ACOG) continues to recommend taking caution to protect both patients and staff against possible COVID-19 exposure during prenatal care appointments. They also recommend we continue to save in-person appointment times for high-risk patients and those requiring additional tests and procedures. At this time, the preterm birth rates in Europe have decreased over the past year; however, in the United States they continue to remain stable (ACOG, 2021).
As NICU nurses, we should try our best to comfort pregnant people as they navigate pregnancy during a pandemic and emphasize the importance of routine antenatal care. Only time will tell if there will be an impact on future NICU admissions.
References:
American College of Obstetricians and Gynecologists. (2021). COVID-19 FAQs for obstetricians-gynecologists, obstetrics. Washington, DC: ACOG; 2020. Available at: https://www.acog.org/clinical-information/physician-faqs/covid-19-faqs-for-ob-gyns-obstetrics. Retrieved April 10, 2021.
Brewster, A. (2020). This is how prenatal care is changing because of coronavirus. Retrieved April 10, 2021, from https://www.todaysparent.com/pregnancy/being-pregnant/prenatal-care-changing-because-of-coronavirus/
World Health Organization. (2016). WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization.
March 2021 - Maryland's Maternal Child Health Initiative: Learning From the Journey
Julie E. Williams, DNP CRNP NNP-BC
From 2019 through March 2021, there were 54 laws enacted across the United States related to maternal and infant mortality and morbidity. In July 2019, the Maryland General Assembly joined the fight and created the Task Force on Maryland Maternal and Child Health under Chapter 661 and 662 of the Acts of 2019 (House Bill 520/Senate Bill 406). The Task Force's goal was to study and make recommendations on maternal-child health, care coordination, and the metrics and finances related to the mother, child, and family (Task Force on Maryland Maternal and Child Health, 2020).
In 2020, the Task Force successfully identified and presented nine recommendations. The recommendations focused on facilitating health care collaboration of critical stakeholders, investing in health improvement, addressing health care disparities, and decreasing health care costs for Marylanders. Key components of the proposal included creating additional workgroups to keep the identified health care efforts moving forward and making a third population health goal.
Background
In 2019, 12.3% of Maryland children lived in families with income below the federal poverty level. The heaviest concentration (31%) of impoverished children were in Baltimore City, which was 80% Black and Hispanic (Kids Count Data Center, n.d.). Food and housing insecurities play a role in the stress and health outcomes of mothers and their children. Research has indicated that an individual's health trajectory over the life span is influenced by early health conditions, including maternal health, in utero conditions, and childhood experiences (Halfon, Forrest, Lerner, & Faustman, 2018). These early experiences can lend themselves to long-term health conditions, including hypertension and obesity.
Compared to other industrialized countries, the United States has a higher maternal and infant mortality rate, with each health outcome exhibiting a significant racial/ethnic disparity. From 2013 to 2017, Maryland's maternal mortality rate was 24.8 maternal deaths per 100,000 live births. During this time, African Americans experienced a rate of almost four times that of Whites (44.7 vs. 11.3 maternal deaths per 100,000 live births) (Maryland Department of Health, 2019). Identification of the disparities is essential, but laws, interventions, and measures to mitigate these disparities are more critical.
Discussion
Under the Maryland All-Payer Model, hospitals are incentivized to support population health. To date, the majority of population health efforts have focused on adults. In fact, two of the three state population goals identified (diabetes and opioid/substance use disorder) do not consistently incorporate strategies that target the maternal-child health population, if at all. While the Task Force realized many successes, one significant achievement is the instatement of Maternal and Child Health as the third total population health goal. More specifically, the goal is to reduce the severe maternal morbidity (SMM) rate by 19% by 2026, with a decrease in Black Non-Hispanic SMM rate by 20% and White Non-Hispanic SMM rate by 15%. Interventions will include a focus on improved preconception health, improved postnatal care, and follow-up.
Despite many interventions and the long history of legal efforts to improve maternal and infant morbidity and mortality, the United States continues to be plagued by high SMM rates. The work Maryland has done to date to prioritize the unique needs of Maternal and Child Health can hopefully encourage other states to do the same. As a nurse working directly with this population, it is imperative to determine the SMM rates within your state and to advocate for the needs of mother and baby. Identify what measures are already in place in your state and what steps can be taken to reduce maternal and infant morbidity and mortality. As a nursing community, we can hopefully come together to influence policy and interventions that will have a lasting positive impact on mothers and children in our communities.
References:
Task Force on Maryland Maternal and Child Health. (2020, August 18). Task Force on Maryland Maternal and Child Health Final Progress Report. Retrieved from Chapter 661 and 662 of the Acts of 2019 (House Bill 520.Senate Bill 406): https://hscrc.maryland.gov/Documents/Maternal%20Task%20Force/Chapters%20661%20and%20662%20of%20the%20Acts%20of%202019%20(House%20Bill%20520.Senate%20Bill%20406)%20%E2%80%93%20Final%20Progress%20Report%20of%20TF%20on%20MD%20MCH.pdf
Kids Count Data Center. (n.d.). Child Population by Race/Ethnicity. Retrieved March 22, 2021, from The Annie E Casey Foundation Kids Count Data Center: https://datacenter.kidscount.org/data/tables/6949-child-population-by-race-ethnicity?loc=22&loct=3#detailed/3/106/false/1729,37,871,870,573,869,36,868,867,133/4406,3303,3304,2161,3305,3306,3307,3301,2796/14060,14061
Kids Count data center. (n.d.). Children in Poverty | Kids Count Data Center. Retrieved March 22, 2021 from KIDS COUNT data center: A project of the Annie E. Casey Foundation: https://datacenter.kidscount.org/data/tables/4460-children-in-poverty?loc=22&loct=2#detailed/2/any/false/1729,37,871,870,573,869,36,868,867,133/any/10017,10018
Halfon, N; Forrest, CB; Lerner, RM; Faustman, EM. (2018). Handbook of Life Course Health Development. Cham: Springer International Publishing.
Maryland Department of Health. (2019). Maryland Maternal Mortality Review. Baltimore: Maryland Department of Health. Retrieved March 22, 2021 from https://phpa.health.maryland.gov/mch/Documents/Health-General%20Article,%20%C2%A713-1207,%20Annotated%20Code%20of%20Maryland%20-%202019%20Annual%20Report%20%E2%80%93%20Maryland%20Maternal%20Mortality%20Review.pdf
February 2021 - From vaccines to masks, where are we now?
Michele A. Sweet, MS RN CCNS
Despite advances in the development of COVID-19 vaccines, January 2021 marked the deadliest month yet of the pandemic in the U.S., with more than 92,000 COVID-related deaths reported. It has become almost a daily routine to look at COVID case numbers and updates from the Department of Health and the Centers for Disease Control (CDC). The incidence of COVID fluctuates by region, in part due to differing vaccine rollouts and mask mandates. Let's take a look at the information offered on vaccines and masks.
100 million vaccines have been administered in the U.S. as of the time of this writing, with 1.6 million additional shots administered daily. Two vaccines are now being offered – from Pfizer and Moderna – and a third vaccine, from Johnson and Johnson, is pending FDA approval. The route and efficacy differ by the vaccine type: Pfizer's requires two injections 21 days apart and reports 95% efficacy preventing symptomatic COVID. Moderna's requires two injections 28 days apart and reports 94.1% efficacy preventing symptomatic COVID. Johnson and Johnson's requires one injection and reports 66-85% efficacy against moderate-to-severe infections.
Vaccination started in December, with health care professionals taking priority, followed by the elderly and those living in long-term care facilities. Since vaccination started, there have been many conversations surrounding the vaccines themselves, with reports of some vaccine hesitancy and racial gaps in vaccine access. States vary in approach and staging for distribution, along with the efficiency and equity of the process. Despite the variance in vaccine role out, almost daily you see postings of individuals being vaccinated on social media. For many, it appears to be a badge of honor to receive the vaccine. It can represent joy, relief, emotions reflecting the loss of a loved one to COVID, and hope for returning to the classroom or office.
As we pass the milestone mark of one year since the first reported COVID case in the United States and initiation of mask-wearing, 15 states and territories do not have mask mandates, and four states that previously had mask mandates have lifted them. Areas with a mask mandate are seeing an overall decrease in COVID-19 cases, while areas that do not have a mask mandate continue to see increases in cases (Hubbard, 2021).
On February 1st, President Biden ordered the first federal mandate for masks to be worn in all federal buildings. The CDC subsequently issued an order requiring the use of face masks on nearly all forms of public transportation (CDC, 2021 Requirement). Dr. Anthony Fauci has even recommended wearing two masks in public. Double masking is suggested as a disposable or surgical mask underneath a cloth mask. A new study published by the CDC in February found that wearing two masks is more effective at preventing coronavirus transmission than one, and significantly boosts protection against the virus (Ries, 2021).
Even after being vaccinated, we are advised to continue to mask because we could still potentially spread the virus if exposed to the disease. The CDC has stated, "Clinical trials of the Pfizer/BioNTech and Moderna vaccines found that both do a good job preventing symptomatic COVID-19 disease, including severe COVID-19. However, the trials did not measure whether a person who is vaccinated is less likely to spread the virus to someone else" (CDC, 2021 Key things).
For some, the yearlong mask-wearing is leading to mask fatigue, particularly for those of us who wear masks all day at work in addition to outside the professional setting. Knowing that you are not alone when it comes to suffering mask fatigue can help. Many articles and self-help tips are being shared by nursing publications, professional societies, newspapers, and psychiatrists. Some of these articles cover how to have a conversation about wearing masks with suggested scripting i.e. "It would really make me more comfortable if we all kept our masks on when we're in this room." While mask-wearing can sound tedious, it can be fun to wear your favorite sports team, animal, or nursing association on a mask. The Ohio State University College of Nursing's Mask Up/Mood Up campaign (The Ohio State University, 2021) encourages deep abdominal breathing upon placement of a mask on your face, and subsequently practicing kindness to yourself and others, with affirmation and gratitude.
Nurses are one of the most trusted professions out there, and we continue to lead the way during this pandemic. Remain informed about your state's vaccine initiatives and spread the word on mask-wearing. Remember to take care of yourself during the pandemic, stop the spread, and spread the word!
References:
Hubbard, K. (2021, February 12). These states have mask mandates. US News and World Report. https://www.usnews.com/news/best-states/articles/these-are-the-states-with-mask-mandates
Centers for Disease Control and Prevention. (2021, February 10). Requirement for face masks on public transportation conveyances and at transportation hubs. https://www.cdc.gov/coronavirus/2019-ncov/travelers/face-masks-public-transportation.html
Ries, J. (2021, January 25). Why you should double-mask to prevent COVID-19. Huffington Post. https://www.huffpost.com/entry/why-double-mask-prevent-covid_l_600f3e87c5b600a27962329e
Centers for Disease Control and Prevention. (2021, February 9). Key things to know about COVID-19 vaccines.
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/keythingstoknow.html
The Ohio State University. (2021, February 4). Mask on/mood up campaign launches to reduce stress and boost mood. Health and Wellness, Chief Wellness Officer.
https://wellness.osu.edu/chief-wellness-officer/mask-mood
Resources:
ANA Enterprise. (2021, February 5). COVID-19 vaccine frequently asked questions.
https://www.nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/coronavirus/what-you-need-to-know/covid-19-vaccines/vaccine-faqs/
Carlsen, A and Huang, P. (2021, February 18). How is the COVID-19 vaccination campaign going in your state? NPR.
https://www.npr.org/sections/health-shots/2021/01/28/960901166/how-is-the-covid-19-vaccination-campaign-going-in-your-state
Centers for Disease Control and Prevention. (2020, December 30). How CDC is making COVID-19 vaccine recommendations
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations-process.html
Greenhouse, S. (2020, July 30). The coronavirus pandemic has intensified systemic economic racism against Black Americans. The New Yorker. https://www.newyorker.com/news/news-desk/the-pandemic-has-intensified-systemic-economic-racism-against-black-americans
Harvard Health Publishing. (2021, February 18). Coronavirus resource center; as coronavirus continues to spread, many questions and answers. https://www.health.harvard.edu/diseases-and-conditions/coronavirus-resource-center#:~:text=The%20answer%20is%2C%20we,virus%20to%20someone%20else
Markowitz, A. (2021, February 17). State-by-state guide to face mask requirements. AARP.
https://www.aarp.org/health/healthy-living/info-2020/states-mask-mandates-coronavirus.html
The Ohio State University. (2021, February 10). How to talk to coworkers who aren't following safety guidelines. FirstUp. https://onfirstup.com/ohiostate/ohiostate/contents/24298531?tok=8b725d11-f511-40bc-9742-57532bc2cc94_3122438
US Department of Health and Human Services. (2021, February 5). COVID-19 vaccines.
https://www.hhs.gov/coronavirus/covid-19-vaccines/index.html
January 2021 - Maternal Access to Mental Health Care: A NICU and National Priority
Susie Taylor, BSN RNC-NIC
Access to mental healthcare for postpartum women must be a priority. One in seven women in the United States will suffer from postpartum depression (PPD) and anxiety disorders. PPD and anxiety can range from mild to severe and can impact not only the mother but the entire family (Feldman, 2020). The American College of Obstetricians and Gynecologists (ACOG) recommends that women receive at least one screening for PPD and anxiety disorders during the perinatal period, usually at their 6-week appointment (ACOG, 2015). Mothers with PPD or anxiety often begin showing signs 1 to 3 weeks after delivery, but symptoms can occur up to one year after childbirth (ACOG, 2015). Mothers with PPD exhibit signs of exhaustion, disengagement with their infant, restlessness, severe anxiety or panic attacks, inability to sleep, or thoughts of harming oneself or baby (mayoclinic.org). Research shows that untreated PPD and anxiety disorders can last longer and have a larger impact on the family unit if not addressed. Children of mothers with untreated PPD are shown to have an increased risk of social emotional disorders, a harder time sleeping, slower weight gain, and delays in language development (mayoclinic.org). Since PPD can impact the entire family and the growth and development of children, the American Academy of Pediatrics recommends routine screening of mothers during the 2-week, 1-, 2-, 4-, and 6-month routine well child visits (AAP, 2020).
Risk factors for PPD are a history of depression, stressful events during pregnancy, traumatic deliveries, low socioeconomic status, poor access to support systems, and babies who have health problems or special needs (mayoclinic.org). While 10% to 15% of postpartum mothers may experience PPD, it is important to note that studies show this number increases to 20% to 35% with NICU admissions (Lean, Rogers, Paul, Gerstein, 2018). During these heightened times of stress, fear, and often isolation from routine life, parents are at a greater risk for PPD and need for intervention. NICU mothers often experience a sense of loss. They have limited control over the care of their infant which can impact bonding. They are sharing precious time with strangers rather than family. When you couple the stress of a hospitalization, with the knowledge that the prime time to assess and intervene for new mothers is at well child visits that are not occurring due to hospitalization, it is easy to see how the mental health of new mothers in the NICU can be overlooked. In addition, it is important to note that women from minority groups are less likely to seek treatment for PPD disorders and if they do are also less likely to follow up with referral care, leaving them at higher risk for repeated depression (Feldman, 2020).
So how can we, as healthcare providers in the NICU, help? We can look for signs of depression or anxiety in new moms (and dads), normalize PPD and anxiety, and verbalize the importance of seeking treatment for the sake of not only the mom, but the baby as well. It is important to work closely with multidisciplinary teams to ensure the whole family unit is being cared for.
We can also advocate for our patients and their families on the national level. In 2019 and 2020, Congress began work on a number of bills aimed at increasing healthcare access for postpartum mothers and children. As the 117th Congress gets underway, we can advocate for the work started to not be forgotten. Bills such as the Helping MOMS Act (H.R. 4996) would extend Medicaid and CHIP eligibility to one year postpartum, allowing mothers to receive continued treatment beyond their delivery. We can advocate for the Black Maternal Health Momnibus Act of 2020 (H.R. 6142) to pass and focus on programs that address the social determinants of health for pregnant and postpartum women. H.R. 6143 (the Moms MATTER Act of 2020) establishes a Maternal Mental and Behavioral Health Task Force to address prenatal and postpartum depression, anxiety, and substance use disorder, with a focus on minority women who are at higher risk for PPD.
Access to mental healthcare for postpartum women must remain a priority in our units and at the national level. Together we can improve mental health access for our patients and families.
References:
Feldman N. Pattani A (2019, November 29). Black Mothers Get Less Treatment for Postpartum Depression. National Public Radio. https://www.npr.org/sections/health-shots/2019/11/29/760231688/black-mothers-get-less-treatment-for-their-postpartum-depression
American College of Obstetrics and Gynecologists. (2021, January 26). Postpartum depression. https://www.acog.org/womens-health/faqs/postpartum-depression
American Academy of Pediatrics. (2021, January 26). Perinatal depression. https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Screening/Pages/Maternal-Depression.aspx
Mayo Clinic. (2021, January 26). Postpartum depression. https://www.mayoclinic.org/diseases-conditions/postpartum-depression/symptoms-causes/syc-20376617
Lean, R. E., Rogers, C. E., Paul, R. A., & Gerstein, E. D. (2018). NICU Hospitalization: Long-Term Implications on Parenting and Child Behaviors. Current treatment options in pediatrics, 4(1), 49–69. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5986282/
Center for Disease Control and Prevention. (2021, January 26). Depression among womenhttps://www.cdc.gov/reproductivehealth/depression/index.htm
December 2020 - Nurses in Congress: Providing Nurses a Seat at the Table
Michelle Cherry, RN DNP
Nurses have a unique perspective into the needs, struggles, and hopes of their patients and patients' families. This inimitable insight makes nurses incredibly valuable at any table, including those of the United States Congress. Nurses are encouraged to become politically active in order to optimize care and health outcomes for neonates and their families and to reduce health care disparities. Nurses have historically stepped into leadership roles at the federal level and we are happy to report that this tradition will continue as a result of the recent national elections.
I am proud of the nurses who have stepped forward to ensure that our important perspectives are heard and that our patients are advocated for. When we think of a nurse who has stood out as the pioneer for nurses' representation in the Federal Government, Congresswoman Eddie Bernice Johnson, RN BSN MPA (D-TX-30) comes to mind. Congresswoman Johnson was the first nurse ever elected into Congress in November 1992 and is currently serving her 14th term. She won this year's election with 78% of the votes. Congresswoman Johnson achieved a lot of firsts upon her congressional election, including being the first chief psychiatric nurse of Dallas; first African American elected to the Texas House of Representatives from Dallas; first woman in Texas history to lead a major committee of the Texas House of Representatives; and the first African American appointed regional director of U.S. Department of Health, Education, and Welfare. (Pollitt, 2020)
Another nurse reelected to office in this cycle is Congresswoman Lauren Underwood (D-IL-14). She was sworn into the 116th U.S. Congress on January 3, 2019. She is the youngest African American woman to serve in the United States House of Representatives. Her motivation to join the congressional race was to protect health care for those specifically with pre-existing conditions. She signed onto the Title VIII nursing reauthorization legislation. Congresswoman Underwood serves on the House Committee on Education and Labor, the House Committee on Veteran's Affairs, and the House Committee on Homeland Security. She also serves on the House Democratic Steering and Policy Committee. (About: Lauren Underwood, 2020). She won this year's election with a close 50.7% of the vote.
Congresswoman Karen Bass (D-CA-37) began her political career representing the 47th district in the California State Assembly (2004–2010). Bass started her professional career as a licensed vocational nurse before becoming a physician assistant (PA), and she was the first PA ever elected to Congress. She was elected to serve as the 67th Speaker of the California State Assembly in 2008 and became the first African American woman in U.S. history to serve as a Speaker of a state legislative body. She was the U.S. Representative for the 33rd congressional district from 2011 to 2013. She currently serves California's 37th congressional district and has served her district since 2013. She won this year's election with 85.9% of the vote. She is chair of the Congressional Black Caucus, Chair of the United States House Foreign Affairs Subcommittee on Africa, Global Health, Global Human Rights, and International Organizations, and United States House Judiciary Subcommittee on Crime, Terrorism, and Homeland Security.
Other notable nurses who have helped pave the way for nursing representation in Congress are Rep. Lois Capps (D-CA) who served from 1998 to 2017, and Rep. Peggy Wilson (R-AK) who served on North Carolina's House of Representatives 25th district from 1989 to 1993. In 2001, Wilson was elected to Alaska's 2nd District House of Representatives and served from 2001 to 2013 and the 33rd district from 2013 to 2015. Rep. Elizabeth Dennigan (D-RI) served her district from 1996 to 2009 and is not only a nurse but a lawyer as well.
As nurses, we took an oath to advocate for our patients, and what better way to achieve that than by seeking elective offices. These opportunities would provide the most impact on giving others a glimpse into the daily challenges nurses struggle to overcome when caring for their patients as well as the challenges our patients face in navigating the health care system.
Read more about NANN's advocacy efforts and resources.
References:
About: Lauren Underwood. (2020, January 28). Retrieved December 07, 2020, from https://underwood.house.gov/about
Clavreul, G. (n.d.). Vote For A Nurse! Retrieved November 03, 2020, from https://www.workingnurse.com/articles/Vote-For-A-Nurse
Nurses Serving in Congress. (n.d.). Retrieved November 03, 2020, from https://www.nursingworld.org/practice-policy/advocacy/federal/nurses-serving-in-congress/
Pollitt, P. (2020, February 01). Nurses in Congress: Eddie Bernice Johnson. Retrieved November 03, 2020, from https://minoritynurse.com/nurses-in-congress-eddie-bernice-johnson/
September 2020 - Make Plans to Cast Your Vote
Michele A Sweet, MS RN CCNS-Neo
Where will you be on Election Day, November 3rd, 2020? None of us can be sure, but we encourage all NANN members to take a little time now to explore the candidates and the issues and to make plans to cast your vote in November.
The United States has a participatory democracy and representative government. Voting is not only a right but a responsibility. The ultimate job review you can give your public officials is by voting – either returning them to office or ending their service. Every vote matters when advocating for the healthcare policies needed to support our profession, our neonates, and their families. Effective advocacy begins with an understanding of the core issues and positions influencing nursing practice at the state and federal level. Not sure where candidates stand on certain issues? Not sure where you are going to be on Election Day? Check out your state legislature's website, the American Nurses Association election information site – www.nursesvote.org, The March of Dimes' advocacy page, and various social media sites that make educating yourself about healthcare policy and candidates easy. Also, take time to learn about casting an absentee ballot in your state, so that no matter where you are on Election Day your voice will be heard.
Nurses are 4 million strong across the U.S. and are the heartbeat and pulse of many communities. By some estimates, 1 out of every 45 potential voters is a nurse. Nurses are advocates for themselves, their own families, their communities, and the neonatal population and families they serve. With the 100th anniversary of the passing of the 19th Amendment (ensuring women the right to vote), we are reminded of the work undertaken by our ancestors, and the nurses before us, who helped make voting an equal right for all. Nursing leaders of the past – Florence Nightingale, Clara Barton, and Dorothea Dix – established a historical foundation that continues to impact nurses today. Nurses in Congress today (Eddie Bernice Johnson [D-TX] and Lauren Underwood [D-IL]) and in the past like Lois Capps who established the Nursing Caucus, have been involved in important discussions involving Medicare, mental health care, opioid safety, safe staffing, and nursing workforce issues to name a few.
Want to learn more about how you can increase your influence on these important issues? Check out the resources on NANN's advocacy page.
The year 2020 has involved ultimate challenges in healthcare. Nurses can help make an impact on the health care that influences their patients and families by either casting an absentee ballot and/or making arrangements to vote early or on Election Day. No matter how you decide to vote, let your voice be heard! Many state deadlines to register to vote or request an absentee ballot are approaching. Check if you are registered so you can be part of the November election.
August 2020 - Advocating for the Rights of Breastfeeding Mothers
Michelle Cherry, RN DNP
With the month of August coming to a close, it felt fitting to reflect on policy and advocacy endeavors surrounding breastfeeding, since August is Breastfeeding Awareness Month. The purpose of Breastfeeding Awareness Month is to promote breastfeeding and raise awareness of the importance of breastmilk/breastfeeding. Feeding breastmilk to infants has an impact on both long- and short-term health outcomes for the infant. Breastfed babies have been shown to have lower incidence of otitis media, urinary tract infections, episodes of diarrhea, and a lower risk of sudden infant death syndrome (SIDS) (Belay, Allen, Williams, Dooyema, & Foltz, 2013). In addition, breastfed infants have lower medical costs due to needing fewer provider visits, hospitalizations, and prescriptions. Breastfeeding also provides benefits to the mother such as, return to pre-pregnancy weight and a reduced risk of breast cancer and osteoporosis. Early and exclusive breastfeeding positively impacts childhood survival in terms of brain development, cognitive performance, and educational achievement seen at age 5 (UNICEF: Breastfeeding, 2015). Breastmilk is the most complete form of nutrition for infants, therefore, interventions that improve breastfeeding rates need to be explored and implemented in order to improve the overall health of our population ("Maternal, Infant, and Child Health," 2016).
One of the provisions of the Affordable Care Act (ACA), Section 4207, amends the Fair Labor Standards Act (FLSA) of 1938 which requires employers to provide each employee reasonable time to express her milk for her child through the age of one. The employer is not required to pay the employee for this time, but the time must be made available. In addition, employers with more than 50 employees are required to provide a place for employees to express breast milk (other than a bathroom). The ACA also requires new private health insurance plans to cover some women's preventative services such as breastfeeding support, supplies, and lactation counseling.
In July 2019, Congress passed the Fairness for Breastfeeding Mothers Act which requires certain public health buildings to provide a clean space, other than a bathroom, which contains a chair, an electrical outlet, and a workable surface for the public to express milk.
When it comes to supporting breastfeeding on a state level, there are areas of the country that excel and areas where we still have opportunities for growth.
Where we excel:
- Women can breastfeed in any public or private location in all 50 states, including the District of Columbia, Puerto Rico, and the Virgin Islands.
Where our opportunities lie:
- Public indecency laws that exempt breastfeeding exist in only 32 states, the District of Columbia, Puerto Rico, and the Virgin Islands.
- Laws that relate to breastfeeding in the workplace exist only in 32 states, the District of Columbia, and Puerto Rico.
- Breastfeeding mothers are exempt from jury duty (or their time may be postponed) in only 19 states and Puerto Rico.
- Breastfeeding awareness educational campaigns have been implemented in only 6 states and Puerto Rico.
Where does your state stand on these issues? Write your congressman and advocate for better amenities for our mothers to ensure their long-term success and improve health outcomes for both mom and baby.
References:
Belay, B., Allen, J., Williams, N., Dooyema, C., & Foltz, J. (2013). Promoting Women's Health in Hospitals: A Focus on Breastfeeding and Lactation Support for Employees and Patients. Journal of Women's Health, 22, 1-4. doi:10.1089/jwh.2012.4040
Maternal, Infant, and Child Health: Objectives. (2016). Retrieved from https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health/objectives
Maternal, Infant, and Child Health: Overview. (2016). Retrieved from https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health
Tahra Johnson, K. B. (2020, July 9). Breastfeeding State Laws. Retrieved August 23, 2020, from https://www.ncsl.org/research/health/breastfeeding-state-laws.aspx
UNICEF: Breastfeeding. (2015). Retrieved from http://www.unicef.org/nutrition/index_24824.html
July 2020 - COVID-19 Bias and Anti-Racism Training Act
Susie Taylor, BSN RNC-NIC
The COVID-19 pandemic has been wreaking havoc for four months, and the call for racial justice in the nine weeks since George Floyd's death has brought our country to the precipice of life-altering change. As members of the sacred nursing profession, we are called to encourage, influence, and be the change needed. NANN has already started this process for change by sharing the message from American Nurses Association president, Ernest J. Grant, PhD RN, and his charge to not only educate yourself but to also "use your trusted voice" to drive change.
Now, we nurses have another opportunity to support positive change, thanks to Representative Alma S. Adams and Senator Kamala Harris' COVID-19 Bias and Anti-Racism Training Act. This legislation aims to directly improve the care that people of color receive through targeted education of health care providers about how to check their own bias and dismantle the systemic racism within our health care structure.
The bill would create a $200 million grant program that would assist with the improvement or establishment of bias and anti-racism training for hospitals, health care providers, medical and professional schools, as well as state and local public health departments. The bill prioritizes funding for the areas of the country that have been hit hardest with the pandemic and are demonstrating high racial and ethnic disparities related to infections, treatment, hospitalizations, and mortality. In addition, the bill requires the Secretary of Health and Human Services to collaborate with health care professionals along with bias and racism policy experts. Together, they would partner with community-based organizations to create evidenced-based training and ongoing education related to bias and anti-racism in health care.
The CDC recognizes that severe illness and death rates tend to be higher for "racial and ethnic minority populations during public health emergencies." COVID-19 is no different, as non-Hispanic Black persons are five times more likely to contract COVID-19, be hospitalized, or die from the disease than non-Hispanic white persons. Hispanic or Latino persons are four times more likely to experience these impacts than non-Hispanic white persons.
Through the support of the COVID-19 Bias and Anti-Racism Training Act and both informal and formal training, nurses across the United States could receive further education on how to acknowledge their own implicit biases and the health care inequities that exist in the United States, and work to eliminate systemic racism. As a nursing organization we stand with the bill sponsors, and health care organizations across the country, to support this bill and advocate for the education to better serve our patients.
In addition to contacting your senator or representative and asking for their support for the passage of the COVID-19 Bias and Anti-Racism Training Act, take time to act now. Educate yourself on the history of systemic racism in the United States and work to immediately improve the care you give daily by educating yourself on your own bias. Resources include:
- COVID-19 Bias and Anti-Racism Training Act of 2020
- NANN's Position Statement on Racial Disparity in the NICU
- Harman, Katharine et al. "Ethnicity and COVID-19 in children with comorbidities." The Lancet. Child & adolescent health vol. 4,7 (2020): e24-e25. doi:10.1016/S2352-4642(20)30167-X
- Kirby, Tony. "Evidence mounts on the disproportionate effect of COVID-19 on ethnic minorities." The Lancet. Respiratory medicine vol. 8,6 (2020): 547-548. doi:10.1016/S2213-2600(20)30228-9
- Evaluate your own bias at https://implicit.harvard.edu/implicit/takeatest.html
June 2020 - Lend Your Voice to Advance Equitable Healthcare
Tommie Farrell, RN
Julie Sundermeier, DNP APRN NNP-BC
According to NANN's 2020 Advocacy Agenda, our organization pledged to support and enhance legislation that would benefit all babies regardless of race, parental economic/educational status, or geographic area. When adding disparities in the NICU to the Advocacy Agenda, no one could have predicted the COVID-19 pandemic or the societal unrest that would follow the death of George Floyd. Both events have highlighted our nation's profound inequalities and the challenges we face in order to create a more equitable world. As nurses, we must hold ourselves, our hospitals, and our governments accountable to the work that needs to be done in order to dismantle the disparities in our NICUs and healthcare systems.
Nurses have the responsibility to look at the healthcare systems we work in and take thoughtful actions to address inequities and advocate for change. A tangible step nurses can take to address the systemic issues we see in our institutions is to engage with elected officials. For 18 consecutive years, Gallup polls have rated nursing as the most trusted profession in the United States. Now is the time to leverage our trusted position, and to lend our voice, expertise, and compassion to educate and bring about the necessary changes to create a more equitable healthcare system.
In a statement to the House Ways and Means Committee on June 1st, President of the American Nurses Association, Ernest J. Grant, PhD RN, called on nurses to "educate yourself and then use your trusted voice and influence to educate others about the systemic injustices that have caused the riots and protests being covered in the news."
"The pursuit of justice requires us all to listen and engage in dialogue with others," he said. "Leaders must come together at the local, state, and national level and commit to sustainable efforts to address racism and discrimination, police brutality, and basic human rights. We must hold ourselves and our leaders accountable to committing to reforms and action."
NANN is aligned with ANA's statement. Our organization understands that nurses can and should lead the charge to create a more just world. Nurses have allies and supporters in Congress, and we must urge them to act too. The Congressional Nursing Caucus is charged with the responsibility of educating elected officials on issues that are important to our profession and how it impacts healthcare. We urge you to review the list of current Caucus Members. If your Representative is not listed, consider sending them a letter urging them to join. This is a great place to start: https://www.aonl.org/advocacy/resources/congressional-nursing-caucus
NANN continues to watch for legislation that will ensure equitable outcomes:
- H.R.1897 MOMMA's Act
- S.116-MOM's Act
- S2373-Rural Maternal and Obstetric Modernization Services Act
We know that there will be more legislation introduced in the weeks and months to come. As a profession, we must reflect on how we can be part of the change in ending systemic racism in our units, hospital systems, and beyond. Change can sound daunting, but a great place to start is in your unit. Read NANN's new position statement, Racial Disparity in the NICU, to learn how you can better support patients and families that face inequality in the NICU. Together we will be able to make great change.
June 2020 - Testing Infants for COVID-19
Raymond K. Riley, BSN RNC-NIC
Health Policy & Advocacy Committee Member
While the COVID-19 pandemic has more significantly affected the adult patient population, especially those with underlying conditions, it is important to take note of the effect the virus has had on the mother/baby dyad. Visiting guidelines have been restricted, mothers and their babies have been isolated from one another, and the continuum of care and childbirth has been interrupted.
There is still a lot to be understood when it comes to infants testing positive for COVID-19 and what protocols should follow. This article does not aim to suggest national guidelines for infants and mothers testing positive for COVID-19, but merely provides examples of what has been done in some NICUs to date, specifically in the region of Washington, D.C., to help nurses navigate the current situation. As NICU nurses, it is our job to stay informed of the most recent guidelines on caring for patients with COVID-19, persons under investigation (PUIs), and their newborn infants. Advocating for patients and their families is more important than ever.
The District of Columbia Department of Health is currently operating under guidelines specified by the CDC. If a pregnant mother tests positive for COVID-19 or gives birth before testing is done and is considered a PUI, then the newborn should also be considered a PUI according to CDC guidelines (Centers for Disease Control and Prevention [CDC], 2020). Infants that are considered PUIs (i.e. born to a mother that is positive or a PUI) will need to be tested to rule out COVID-19 infection (Government of the District of Columbia, 2020). Currently, there is little data available on all the possible routes COVID-19 can be transmitted between a mother and a newborn. The CDC is currently recommending that infants should be separated from a mother that is positive or a PUI to minimize the risk of transmission through respiratory secretions. These infants should also be treated as PUIs until they have negative tests (CDC, 2020).
The process for testing an infant is slightly different than an adult. First, the infant should be bathed after birth to remove any fluids potentially containing the virus from the skin. Infants should be tested at 24 hours of life, and then again at 48 hours of life. To test an infant, one swab is inserted into the throat and then into the nasopharynx. That single swab is placed in the viral transport media and sent to the lab for testing (Cummings et al., 2020). An infant would be considered negative if both tests resulted in undetected for the virus.
In the example of Washington, D.C., on a case by case basis, the government health organization directs facilities to allow infants that are born well and test negative to be kept with their COVID-19 positive mother depending on the mother's wishes, facility constraints, illness severity, and individual needs (Government of the District of Columbia, 2020). The CDC endorses this practice and recommends that any infant that is kept in the same room as a positive mother be behind a physical barrier such as a curtain and maintain a 6-foot distance (CDC, 2020). Infants that test negative, do not require NICU admission, and have a negative adult family member can be discharged home. The infant should remain isolated from any positive family members until they are negative. Finally, infants that test positive or remain PUIs, but have no symptoms and do not require NICU care can be discharged home in some cases. These infants should have thorough follow-up through 14 days after birth, and the caretakers should be instructed to take proper precautions at home including hand hygiene, gloves, and masks (Cummings et al., 2020).
Advocating for patients, families, and keeping the mother/infant dyad together, NANN has released a position statement to guide nurses and institutions during the current COVID-19 pandemic. In accordance with the previously stated CDC guidelines, NANN encourages and fully supports the practice of shared decision making between the mother and the clinical team. This allows the mother to be involved with the decision regarding the plan of care for her infant and develops a working partnership between the two parties. As nurses, we have the opportunity to participate in this holistic approach, determining the plan of care, ensuring that: the family's needs, the infants' needs, and the family's thoughts and feelings are all acknowledged and addressed.
The challenge nurses currently face is immense. To help patients and their families, nurses must try their best to understand the varying and evolving guidelines, recommendations, and the impact protocol may have on a baby and their mother. Together we can learn the best tools for advocating for our mothers and babies during this pandemic.
References:
Centers for Disease Control and Prevention. (2020). Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings.https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html.
Cummings, J., Hudak, M., Kimberlin, D., & Puopolo, K. (2020). Management of Infants Born to Mothers with COVID-19. American Academy of Pediatrics.
Government of the District of Columbia. (2020). Guidance for Pregnant Women COVID19. https://coronavirus.dc.gov/.
National Perinatal Association/ National Association of Neonatal Nurses. (2020). Mothers with COVID-19 and Their Newborn Infants. http://nann.org/uploads/About/PositionPDFS/Position%20Statement%20COVID-19_NPA%20and%20NANN.pdf
April 2020 - Nurses on the Frontline
Julie Sundermeier, DNP APRN NNP-BC
NANNP Council Member
On March 11th, the World Health Organization designated COVID-19 as a global pandemic. In the US, we witnessed the global effects of this virus and continue to experience the impact on society, the economy, and healthcare. Since the first case of COVID-19 was reported in the US on January 11, 2020, the country has reported 938,154 cases, and 53,755 deaths. (John Hopkins University; April 28, 2020). Hospitals across the US, especially in areas hardest hit, have experienced marked shortages of personal protective equipment, testing, ventilators, bed space, and healthcare personnel, including nurses and advanced practice registered nurses (APRNs).
To overcome nursing shortages many states took steps to authorize emergency licensure to provide the increased coverage needed during surge capacity. This involved temporary licensure for retired, out-of-state, and inactive nurses and nurse practitioners (NPs). States have also temporarily waived part of the requirements or all requirements for collaborative/supervisory/protocol agreements for NP practice.
The need for professional mobility in times of crisis brings to light advantages of compact State Licenses for RNs, as well as APRNs. Currently there are 33 States with eNCL (Nurse Licensure Compact) legislation for RNs. New Jersey enacted partial implementation on 3/24/20 and Indiana has future implementation slated for 7/1/20. Nurses apply for their multistate license in their home State, which allows them to practice with one license, either in person or via telehealth, in both their home state and other states participating in the NLC.
A license compact for APRNs was proposed in 2015 by the National Council of State Boards of Nursing (NCSBN). Under the APRN Compact, APRNs could legally provide care to patients across state lines without having to obtain additional licenses. Currently, three states have signed APRN Compact legislation: Idaho, Wyoming, and North Dakota. These states are 3 of the 22 in the nation (plus the District of Columbia) who grant full practice authority. The primary barrier to the APRN Compact moving forward will be individual state legislation and restrictions that are imposed limiting full practice authority. The APRN Compact will be implemented when 10 states have enacted the legislation. In order to be eligible to join the APRN Compact, states must pass the model legislation without any material differences. (NCSBN, 2020).
The benefits of the APRN Compact include:
- Creates a model that allows APRNs to practice freely among member states while still allowing states to retain autonomy and the authority to enforce the state nurse practice act.
- Improves access to licensed APRNs during a disaster or other times of great need for qualified advanced nursing services.
- Benefits military spouses with APRN licenses who often relocate every two years.
- Grants the necessary legal authority to facilitate interstate information sharing and investigations in the event of adverse actions to ensure public protection.
- Eliminates redundant, duplicative regulatory processes and unnecessary fees.
In addition, many states have called for health care volunteers to help respond to the pandemic crisis. American Academy of Nurse Practitioners (AANP) is tracking calls for volunteers and you can find more information about state volunteer opportunities on their website.
The ANA website has a link for volunteer sites for RNs.
Emergency responses to RN and APRN practice and education, as well as state emergency responses, can be found at https://www.ncsbn.org/14508.htm. National Conference of State Legislatures is tracking state actions related to licensed workers as part of the COVID-19 response:
*eNLC states for RNs include: Alabama, Arizona, Arkansas, Colorado, Delaware, Florida, Georgia, Idaho, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Mexico, North Carolina, North Dakota, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, West Virginia, Wisconsin, and Wyoming.
March 2020 - Completing the 2020 Census is More Important than Ever
Susie Taylor, RNC-NIC
NANN HPAC Member
The year 2020 has been declared "The Year of the Nurse and the Midwife" by the World Health Organization and it is also the year for the 2020 United States Census. As nurses it's important to know how the census impacts our federal government, but more important for us is to understand how it will effect healthcare.
Let's start with a quick overview of the basics:
- It is mandated by Article 1 Section 2 of the U.S. Constitution that the population of the United States be counted every ten years. It is vital to get an accurate population count as the U.S. Census helps determine how hundreds of billions of federal dollars will be spent and distributed across the country, including funding for schools, police and fire departments, road and infrastructure projects, and health clinics.
- The 2020 census survey runs from March 12- July 31, 2020 and can be completed online, by phone or in person. In December of 2020 the Census Bureau will give its report to the President and Congress. The 2020 census is being monitored closely to evaluate the need for an extension or change in methodology due to COVID19.
- Based on the number of people counted in each state, changes to the makeup of the U.S. House of Representatives may be adjusted in a process known as reapportionment. Some states will gain an extra congressional representative and others will lose a seat to make up the 435 members of the House of Representatives. The count also impacts the number of Electoral votes each state has in presidential elections.
The census impacts healthcare in a variety of ways. While the census occurs every 10 years, the data taken from it influences the delivery and funding for the healthcare of millions of Americans each year. The Census Bureau is also responsible for the American Community Survey (ACS) to collect socio-economic data of the U.S. population on a yearly basis. With this information the data enables:
- Establishment of eligibility and reimbursement rates set for Medicaid, enrollment for Children's Health Insurance Program (CHIP), and Supplemental Nutrition Program for Women, Infants and Children (WIC).
- Medicare Part B reimbursement rates to be set, and an account for the cost of providing care in specific geographical areas.
- Social Determinates of Health. The 2020 Census tracks the population's race, nation of origin, and type of housing. The ACS expands on the census by evaluating income and educational levels on a yearly basis in order to understand where/what resources are needed most. All of these factors are known to be influencers of health.
- Public Health Measures. The CDC and Department of Health and Human Services utilize census results for research, tracking diseases, and potential barriers to federal program access. Without an accurate count of the population, how could the CDC truly know the impact of a disease such as the yearly flu or the current COVID19?
The 2020 Census is open! Go to https://2020census.gov/ to respond today or to learn more.
References:
https://2020census.gov/en/census-data.html
Leadership Conference Educational Fund, April, 2018, The Census and Healthcare. Center on Poverty and Inequality, Georgetown Law https://censuscounts.org/wp-content/uploads/2019/03/Census-Health-Care-Factsheet.pdf
March 2020 - 2020 Advocacy Agenda
As the association for neonatal nurses and advanced practice neonatal nurses, NANN seeks to optimize care and health outcomes for neonates and their families. In an initiative to be purposeful with our legislative advocacy efforts, the Health Policy and Advocacy Committee has created an advocacy agenda for the year. We will focus our energy, communication channels, and resources towards advancing our core issues at the federal level. The full agenda follows and an electronic copy is available.
Disparities in the NICU
There are numerous studies demonstrating health disparities in pre-term NICU infants. Three contributors to health disparities have been described: increased risk for pre-term birth, lower quality of care, and socioeconomic disadvantages. NICU mothers who experience poor social determinants of health have an increased risk of losing a child before his or her first birthday. NANN strongly believes that all infants, regardless of race, parental economic or educational status, or geographic area should receive equal, quality healthcare.
Related legislation:
S. 2373 – Rural Maternal and Obstetric Modernization Services Act
Paid Family Leave
Paid family leave allows working people to continue to earn all or a portion of their income while they take time away from work to meet family caregiving or personal health needs. This can include time to address a serious medical condition or a significant health event such as pregnancy (medical) and to care for a newborn. Paid leave is a critical tool to invest in the mother and infant needs, supporting healthier pregnancies, better birth outcomes, more successful breastfeeding, and both physical and mental health in the post-partum period.
Related legislation:
H.R. 4964 – Paid Family Leave Pilot Extension Act
Nutrition and Breastfeeding
The breastfeeding experience plays an important role in the healthy neurological development of the infant as well as supporting the establishment of the critical relationship between the infant and mother as a dyad. NANN supports the need for access and education to information on breastfeeding, thereby encouraging breastfeeding as the best possible experience for the nutritional and emotional health of infants.
Related legislation:
H.R. 5592 – PUMP for Nursing Mothers Act (S. 3170 Companion Bill)
S. 2381 – Traveling Parents Screening Consistency Act of 2019
Nursing Workforce Development
The continued development of the nursing workforce is critical to the health of our country. Through research, education, expansion of access to healthcare facilities and providers, and funding directly connected to meeting the nursing profession's pressing needs, NANN advocates for the entire nursing community.
Related legislation:
H.R. 728 - Title VIII Nursing Workforce Reauthorization Act of 2019 (Passed House)
S. 1399 – Title VIII Nursing Workforce Reauthorization Act of 2019
S. 1045 – Nursing Where It's Needed Act
H.R. 900 – ACO Assignment Improvement Act of 2019
NANN will continue to provide updates and calls to action regarding our 2020 Advocacy Agenda priorities.
February 2020 - The First 1,000 Days
Michelle Cherry, DNP RN
Children and their mothers have struggled with obtaining adequate nutrition throughout the world and many suffer from chronic malnutrition leading to their developmental growth being stunted. Chronic malnutrition has downstream effects on these children and often lead to life-threatening diseases and infections. Obesity is another form of malnutrition that has affected our youth, mainly due to unhealthy diets.
The United States is one of the wealthiest nations in the world yet still suffers from having one of the highest infant and maternal mortality rates. The U.S. statistics are staggering with:
- 1 in 12 babies being born at low birth weight
- 1 in 6 have not had any breastmilk
- 1 in 4 being overweight/obese by the time they turn 5
- 1 in 6 under 6 years old live in households that struggle with healthy food options.
Contributing to high obesity rate, the U.S. has one of the unhealthiest diets which is high in sugar and saturated fats and low in fruits and vegetables. The population most affected by these low nutritional diets are low-income families. These differences in healthy food intake habits widen the gap with already existing disparities.
Where do we go from here to look to improve the outcomes of our new moms and babies? Supporting the mother's nutritional status during pregnancy is key in ensuring her diet can support the needs of her fetus's rapidly growing brain. The mother requires foods that are rich in folic acid, zinc, iron, and iodine, as well as protein and fatty acids to support this growth. Lack of any of these critical nutrients can lead to developmental delays, cognitive deficits, and birth defects.
During the first 1,000 days of a newborn's life, their brain is growing faster than any other period. The nutritional status of the mother and baby are stepping-stones in building baby's cognition and motor skills. Without proper nourishment and nutrition, the baby's ability to reach developmental milestones is hindered, creating irreversible damage to their growing brain. Once the damage is done, it cannot be reversed and is the reason that the first 1,000 days of life are so important. Breastmilk contains the perfect nutrition to support brain growth and provides nutritional support that formula cannot replicate, such as growth factors and hormones. It is no surprise that breastfed babies perform better on intelligence tests and have higher IQ scores. Breastfeeding also provides physical contact that supports the baby's sensory and emotional needs. Rapid brain growth reaches 80% by age 3 and 90% by age 5, and this growth requires foods rich in iron, zinc, and protein. A deficiency in these critical nutrients can impair their learning capacity and their behavior.
1,000 Days is working to turn what the evidence shows as best practices into a reality to improve the lives of these moms and babies. 1,000 Days focus is to:
Increase investment in women's nutrition and health throughout the 1st 1,000 days
Expand programs that provide the most vulnerable children with proper nutrition to ensure they thrive- In December 2019, funding for global nutrition programs was increased by $150 million
Improve baby/toddler diets and feeding practices- Supplemental nutrition programs for WIC will receive $6 billion, and Breastfeeding Peer Counselor Programs will receive full funding of $90 million for the 1st time
Improve policy and funding to ensure that more children are provided with mother's own milk- The CDC received a small increase after years of flat funding to include $9 million aimed at providing hospitals and states with the tools to help improve breastfeeding rates and implement baby-friendly practices.
Calling on Congress and the administration to support a comprehensive paid family and medical leave program that covers all workers
Join the movement to help moms and babies by visiting 1,000 Days website and send a letter to your members of Congress to urge their support in the campaign and for Paid Parental Leave.
Reference:
Homepage- 1,000 Days. (n.d.). Retrieved January 27, 2020, from https://thousanddays.org/
July 2019 - Update on Nurse Practitioner Full Practice Authority in the U.S.
Julie Sundermeier, DNP APRN NNP-BC
The American Association of Nurse Practitioners defines full practice authority as "the authorization of nurse practitioners (NPs) to evaluate patients, diagnose, order and interpret diagnostic tests and initiate and manage treatments—including prescribe medications—under the exclusive licensure authority of the state board of nursing." There are 22 states and the District of Columbia, along with two U.S. territories, who currently have Full Practice Authority (FPA) for nurse practitioners as seen in green on the map below (AANP, 2018). States with a reduced or restricted environment have laws either requiring a career-long regulated collaborative agreement, limits on the setting of one or more elements of NP practice, or delegation and team management by another health provider.
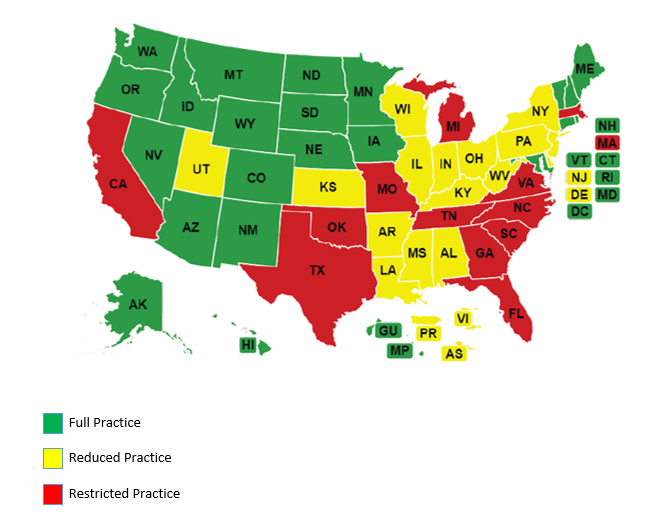
Several states have introduced FPA legislation in 2019 with varying degrees success including California, Florida, Kansas, Indiana, Massachusetts, Ohio, Pennsylvania, North Carolina, Rhode Island, and Wisconsin. As legislation is introduced APRNs are educating legislators and the public on how FPA can improve access to care, reduce cost, and increase efficiency. States are also making incremental advances towards Full Practice Authority. Below are examples of 2019 state legislation regarding prescriptive authority:
- Arkansas - AR H 1267- Enacted March 29. Extends the prescriptive authority of an advanced practice registered nurse to Schedule II drugs, under certain conditions.
- New Jersey - SB 1961 eliminates requirement of joint protocol with physician for advanced practice nurses to prescribe medication.
- Utah - HB 336 signed in to law on March 25. Amends the requirements for NPs to maintain a consultation and referral plan to legally prescribe Schedule II agents. Once enacted, the law narrows this requirement to NPs who open their own practice and who have been licensed as an APRN for less than one year, or who have fewer than 2,000 hours of practice. The new law allows the supervisor of a consultation and referral plan to be either a physician or an APRN who has at least three years of experience. The requirement for a career-long consultation and referral plan for NPs who own or operate pain management clinics remains unchanged.
References:
AANP (2018, December). State Practice Environment. Retrieved from https://www.aanp.org/advocacy/state/state-practice-environment
May 2019 - Two Bills Affecting our Patient Population
Alyssa Jelinek, BSN RNC-NIC
MOMMA Act
Introduced by Representative Kelly (D-IL), the Mothers and Offspring Mortality and Morbidity Awareness (MOMMA) Act overall aims to improve federal efforts in preventing maternal mortality. Within the United States about 700 women die due to pregnancy related complications while another 65,000 suffer near-fatal complications. The United States continues to have a high maternal mortality rate when compared to other countries, it is believed that as many as half of these are preventable. There are also significant racial disparities with Black women dying of maternal-related deaths at three to four times that of non-Hispanic White women; specifically, there are 12.7 death per 100,000 live births for White women, 14.4 deaths per 100,000 live births for women of other ethnicities, and an alarming 43.5 deaths per 100,00 live birth for Black women.
The MOMMA act will address these alarming issues through developing policies to improve data collection, disseminate information on effective interventions, and expand health care and social service access for postpartum women. The MOMMA act would also extend Medicaid, CHIP, and WIC coverage for pregnant and postpartum women from 60 days to 1 year. Finally, this legislation aims to address cultural competency and implicit bias (attitudes or stereotypes that affect our understanding, actions and decisions in an unconscious manner) through education.
Please support the MOMMA Act by following this link to reach out to your Representative and Senators.
H.R. 728: Title VIII Nursing Workforce Reauthorization Act of 2019
Introduced by Representatives Joyce (R-OH), Gabbard (D-HI), Davis (R-IL), Bonamici (D-OR), Matsui (D-CA), Castor (D-FL), McKinley (R-WV), and Underwood (D-IL) on January 23rd, 2019, the purpose of the bill is to amend Title VIII of the Public Health Service Act, extending through Fiscal Year 2024. Specific programs focus on nurse retention, recruitment, education (through advanced education), and faculty preparation.
The new bill proposes amendments to several sections to include:
- An annual report on the nursing workforce programs to be submitted by the Secretary. The purpose of the report is to assess the Department of Health and Human Services' programs and activities to improve the nursing workforce. The report will identify to what extent the programs are meeting their goals.
- Recognition for all advance practice nursing roles with newest addition of clinical nurse specialists; adding the CNS to the current group of nurse practitioners, certified registered nurse anesthetists and certified nurse-midwives.
- Further funding for increasing nursing workforce diversity, giving grants to increase opportunities for students with minority backgrounds.
- Promote a career ladder through supporting career advancement through rewarding grants to promote specialty training as well as baccalaureate and graduate prepared nursing education, among other supportive measures.
- Adds Nurse Managed Health Clinics to list of eligible entities in the definition section
March 2019 - Legislation Affecting Moms and Babies
Theresa Crowe, BSN CCRN
The government has reopened and Congress is back to work. Among the many pieces of legislation that have been introduced for consideration this year, there are a handful that should be of particular interest to health care professionals working with moms and babies.
First, is the Modernizing Obstetric Medicine Standards or "MOMS" Act, introduced by Sen. Kristen Gillibrand (D-NY). This act seeks to provide $5,000,000 a year from 2020-24 to the Maternal and Child Health Bureau of the Health Resources and Services Administration (HRSA) to study, develop, and initiate best practices that would improve the quality and safety of maternity care across the continuum. The end goal would be to decrease the high levels of maternal mortality and morbidity in the United States.
Next, Rep. David P. Joyce (R-OH-14) has introduced H.R. 383, Continuing Coverage for Preexisting Conditions Act of 2019, which, if passed, would maintain the Patient Protection and Affordable Care Act's particular requirement that people could nNAot be denied insurance coverage because of their pre-existing conditions. This is significant for many of our moms seeking prenatal care who have pre-existing conditions such as diabetes, as well as important to many of our babies who will grow up with chronic illnesses. Another bill that would adversely affect access to prenatal care, especially for low-income women, is H.R. 369 Defund Planned Parenthood Act of 2019 as introduced by Representative Vicky Hartzler (R-MO-4).
Finally, there is the Nationally Enhancing the Wellbeing of Babies through Outreach and Research Now or "NEWBORN" Act, introduced by Rep. Steve Cohen (D-TN-9). This would provide HRSA with $10,000,000 each year from 2020-24 to target areas in the United States with the highest rates of infant mortality (city or rural). HRSA would then work with local agencies already in place to fund outreach, education, and treatment programs aimed at decreasing the infant mortality rate in these areas. This systems approach includes efforts to prevent preterm labor, enhance maternal health and address family needs, (including mental health, substance abuse, housing, domestic violence, smoking cessation, access to health care, etc.), as well as education and support for parents on how to care for babies and keep them safe and healthy. This program would also require HRSA to track information on the success of the programs utilized so that in 2024, health agencies will have a better idea where to focus their efforts across the entire country to further decrease our high rate of infant mortality.
Advocate on behalf of your profession!
All of the above pieces of legislation have just been introduced in January 2019. If one of your New Year's resolutions is to become more aware of or active in the issues that affect you and your patients, follow their progress on Congress.gov. You can look up any piece of legislation in either the House or Senate and even apply filters to help you get to specific areas of interest or concern (such as health). In addition, you can always email or call your local representatives to express your support or opposition to these bills (many are co-sponsored by other Congressmen and Congresswomen) or the offices of the individuals listed above who have introduced them.
January 2019 - Meet Your Nurse Representatives in Congress
Tommie Farrell, RNC-NIC
HPAC Board Liaison
The U.S. Government has finally reopened after the longest shut down in history - Congress now has until February 15 to make a deal or risk another shutdown. With Nancy Pelosi (D-CA-12) retaking the position of Speaker of the House, the shutdown represented the new power dynamic at the federal level as the Democrats now control the House of Representatives. The incoming freshmen for the House represents the most diverse class ever.
As for health care, we are seeing more science-based representation. Four RN elected officials bring years of nursing and health care education and expertise with them. It is imperative that the most trusted profession in the country has the ability to advocate for our patients and families, present evidence for the need for adequate health care access, and share our unique perspective on how best to reach and care for underserved populations.
Presently, there are four nurses in Congress.
 U.S. Rep. Eddie Bernice Johnson (D-TX-30), reelected to a 14th term was the first nurse elected to Congress and has been a tireless advocate for nurses on the Hill. She serves on the House Committee on Science, Space, and Technology, as well as serving on the House Committee on Transportation, and Infrastructure. Johnson is also a part of the Nursing Caucus.
U.S. Rep. Eddie Bernice Johnson (D-TX-30), reelected to a 14th term was the first nurse elected to Congress and has been a tireless advocate for nurses on the Hill. She serves on the House Committee on Science, Space, and Technology, as well as serving on the House Committee on Transportation, and Infrastructure. Johnson is also a part of the Nursing Caucus.
 U.S. Rep. Donna Shalala (D-FL-27), Secretary of Health and Human Services under former President Bill Clinton and chair of the 2010 Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing Report at the Institute of Medicine, won a Miami-area congressional seat. Shalala has built a reputation as a staunch supporter of nurses throughout her distinguished career, most recently serving as president of the University of Miami. (Campaign for Action, November, 2018) Shalala serves on the House Committees on Rules and Education and Labor.
U.S. Rep. Donna Shalala (D-FL-27), Secretary of Health and Human Services under former President Bill Clinton and chair of the 2010 Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing Report at the Institute of Medicine, won a Miami-area congressional seat. Shalala has built a reputation as a staunch supporter of nurses throughout her distinguished career, most recently serving as president of the University of Miami. (Campaign for Action, November, 2018) Shalala serves on the House Committees on Rules and Education and Labor.
 U.S. Rep. Lauren Underwood (D-IL-14), is an RN who is the youngest black female to be elected to Congress. Her focus has been on public health policy and she has a strong interest in the Affordable Care Act, focusing on pre-existing conditions. She holds two master's degrees in public health and nursing. Her background includes work with the Obama administration working on public health, emergencies, and disaster response. She has also worked for the Department of Health and Human Services.
U.S. Rep. Lauren Underwood (D-IL-14), is an RN who is the youngest black female to be elected to Congress. Her focus has been on public health policy and she has a strong interest in the Affordable Care Act, focusing on pre-existing conditions. She holds two master's degrees in public health and nursing. Her background includes work with the Obama administration working on public health, emergencies, and disaster response. She has also worked for the Department of Health and Human Services.
 U.S Rep. Karen Bass, (D-CA-37), originally a vocational nurse, moved on to become a physician's assistant. She serves on the House Committee on Foreign Affairs and is on the House Judiciary Committee.
U.S Rep. Karen Bass, (D-CA-37), originally a vocational nurse, moved on to become a physician's assistant. She serves on the House Committee on Foreign Affairs and is on the House Judiciary Committee.
Advocate on behalf of your profession!
These women represent the future of health care. We encourage you to engage with NANN and your elected officials to help shape what the future will look like for the nursing profession, health care policy and our vulnerable patients.
October 2018 - Year in Review
Stephanie M. Blake, DNP APRN NNP-BC
HPAC Chair
CHIP
HPAC continued its reporting on the funding crisis facing the Children's Health Insurance Program (CHIP). CHIP is a grant program in which the federal government and the state's share the cost of extending health insurance coverage to children who neither qualify for Medicaid or whose parents don't have health insurance through their jobs.
Good news for the millions of children covered under this program, CHIP funding has been extended in the federal budget through FY2023. A few highlights of the new funding:
- Provides federal funding for CHIP for six years, from FY2018 through FY2023.
- Continues the 23-percentage point enhanced federal match rate for CHIP that was established by the Affordable Care Act, but reduces the federal match rate to the regular CHIP rate over time.
- Extends the requirement for states to maintain for coverage for children from 2019 through 2023; after October 1, 2019, the requirement is limited to children in families with incomes at or below 300% FPL.
Title VIII
HPAC played a pivotal role in the continued advocacy for this program. Title VIII or the Nursing Workforce Development program funds nursing education helping educate nurses who work in the rural or underserved areas. Additionally, the funds provide loan forgiveness for clinical nurses and nursing educators in order to increase retention within the nursing field. The funds for this program are awarded from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA). The advanced nursing education grants have helped educate nurse practitioners, clinical nurse specialists, nurse midwives, nurse anesthetists, nurse administrators, and public health nurses in primary care in unserved and rural areas. The Fiscal Year 2018 Omnibus Appropriations bill was signed by the President and includes $249.472 million for Title VIII, which is close to a 9% increase over FY 2017. The bill also included $158 million for the National Institute of Nursing Research, which is a 5% increase over FY 2017.
ACA
On June 7th, the Justice Department indicated that it would not defend the Affordable Care Act's (ACA) constitutionality in a case filed by Texas and 19 other states (opposed by 16 other states). The case asserts that because the new Republican tax act removed the individual mandate, the ACA is no longer a constitutional exercise of Congress's power to tax, as established by a 2012 Supreme Court decision. In its statement letter, the Justice Department contends that the ACA provision requiring most Americans to carry health insurance will soon no longer be constitutional and that, as a result, consumer insurance protections under the law will not be valid either – including preexisting conditions coverage. If these provisions of the ACA were to be deemed unconstitutional, it would once again allow insurers to deny or charge more to people with chronic or preexisting conditions.
August 2018 - Affordable Care Update
Theresa Crowe, BSN CCRN
On June 7th, the Justice Department indicated that it would not defend the Affordable Care Act's (ACA) constitutionality in a case filed by Texas and 19 other states (opposed by 16 other states). The case asserts that because the new Republican tax act removed the individual mandate, the ACA is no longer a constitutional exercise of Congress's power to tax, as established by a 2012 Supreme Court decision.
In its statement letter, the Justice Department contends that the ACA provision requiring most Americans to carry health insurance will soon no longer be constitutional and that, as a result, consumer insurance protections under the law will not be valid either – including preexisting conditions coverage. If these provisions of the ACA were to be deemed unconstitutional, it would once again allow insurers to deny or charge more to people with chronic or preexisting conditions.
The removal of such protections may cause new challenges for our patient populations. NANN will continue to monitor and provide up-to-date information as it becomes available.
August 2018 - ANA Hill Day: Nurses Stand Together
Tommie Farrell, BSN RNC-NIC
If you ever want to feel energized and empowered, spend a day in DC with almost 1000 nurses and advocate for our patients, health care and our profession! My colleague, Heather Hopkins (DVANN) and I joined the American Nurses Association (ANA) on the Capital Hill on June 21st to elevate nursing concerns and demonstrate how our collective voices matter in directing healthcare in America.
While on the Hill, we were able to shine a light on critical issues impacting healthcare, our patients, and our nursing practice. Among the topics we spoke about were the Title VIII Nursing Workforce Reauthorization Act, (H.R. 959/ S. 1109), The Safe Staffing for Nurse and Patient Safety Act (H.R. 5052/ S. 2446), and The Addiction Treatment Access Improvement Act of 2017 (H.R. 3692/S. 2317). Many of us had other concerns, not the least of which is the status of families and children caught up in the Immigration debate. So, yes, we dove right in to let everyone know that nurses stand behind the need to protect these vulnerable families.
Because of our advocacy on June 21st, we were able to speak to the importance of APRN prescribing authority regarding MAT (medication assisted treatment). The very next day and directly influenced by our stories, this bill passed through the House and is next up in the Senate. This directly impacts our NAS infant's outcomes for them and their mothers. What a great feeling to have participated in this process!
It is easy to be overwhelmed by our daily lives and feel we don't have time or energy to add advocacy to our list of "to do's" but it is critical for nurse's voices to be heard and to be part of the process. We are the front line for healthcare in America. You certainly don't need to get to DC to do this. Call, email, write and participate in local town halls. Stop by your local offices to check in and tell your story. As we continue to stay involved in advocacy, we look forward to you joining is in the process.
April 2018 - Title VIII Nursing Workforce Development: Small Win and What's Next?
 Michelle Cherry, DNP RN
Michelle Cherry, DNP RN
Now that President Trump has signed the spending bill to fund the government through September: what is the impact on nursing, what is Title VIII funding, and what does it mean to you?
Title VIII or the Nursing Workforce Development program originally began in 1964 by Lyndon Johnson as the Nursing Training Act of 1964 in response to the nursing shortage – more than 20% of hospital nursing positions were vacant. The funds from this program were utilized to fund nursing education and to help educate nurses who work in the rural or underserved areas. In addition, the funds provided loan forgiveness for clinical nurses and nursing educators in order to increase retention within the nursing field. The funds for this program are awarded from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA). The advanced nursing education grants have helped educate nurse practitioners, clinical nurse specialists, nurse midwives, nurse anesthetists, nurse administrators, and public health nurses in primary care in unserved and rural areas.
There are currently an estimated 2.75 million registered nurses in the United States. According to the Bureau of Labor Statistics (BLS), the nursing workforce is projected to increase by 15% between 2016 and 2026 in order to meet the needs of our baby-boomers that are living longer, increased emphasis on preventative care, and to address chronic conditions. Currently, nursing schools are turning away qualified applicants due to lack of faculty, clinical sites, classroom space, clinical instructors, and budget limitations according to the American Association of Colleges of Nursing. In 2016 alone, nursing schools were forced to turn away 64,067 qualified applicants to nursing programs. A report issued by the Bureau of Health Professionals predicts by 2020, the percentage of unfilled nursing positions will increase by 29%.
The Fiscal Year 2018 Omnibus Appropriations bill was signed by the President and includes $249.472 million for Title VIII, which is close to a 9% increase over FY 2017. The bill also included $158 million for the National Institute of Nursing Research, which is a 5% increase over FY 2017. The breakdown of the Title VIII programs are listed. As nurses, we need to continue to speak Congress regarding the importance of these Title VIII funds. NANN will continue to provide updates on Title VIII Nursing Workforce Reauthorization Act of 2017 (HR 959/S.1109).
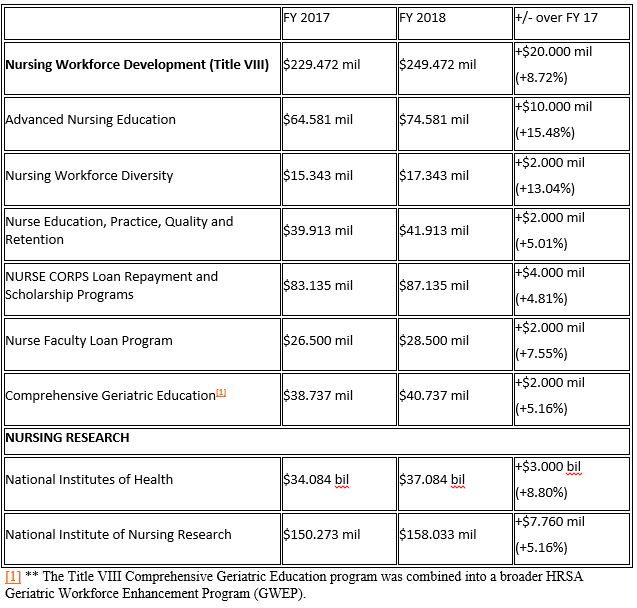
March 2018 - CHIP Renewed Through FY2023
Theresa Crowe, BSN CCRN
Last fall, the Health Policy and Advocacy Committee (HPAC) reported on the funding crisis facing the Children's Health Insurance Program (CHIP). CHIP is a grant program in which the federal government and the states share the cost of extending health insurance coverage to children who neither qualify for Medicaid or whose parents don't have health insurance through their jobs. Information from the Centers for Medicare and Medicaid Services (CMS) indicates that about 9 million kids were covered by CHIP in fiscal year 2016.
Unfortunately, the federal side of CHIP's funding was set to expire this last September. Without that federal funding assistance, states would have been left to their own to either come up with the shortfall elsewhere in their budgets or to no longer offer coverage. Congress had been struggling over the budget, including whether or not to continue to fund CHIP. For these 9 million children and their families, they were facing the prospect of losing their health insurance and being unable to continue to afford much-needed medical care.
Congress provided some temporary stopgap measures to continue CHIP funding until March 2018, a time when it was believed that the final federal government budget plan would be finished. Professional organizations such as NANN, the March of Dimes, The Children's Hospital Association, and many others strongly supported the continuation of CHIP. In an example of successful advocacy, CHIP funding has been extended in the federal budget through FY2023. A few highlights of the new funding:
- Provides federal funding for CHIP for six years, from FY2018 through FY2023.
- Continues the 23 percentage point enhanced federal match rate for CHIP that was established by the Affordable Care Act, but reduces the federal match rate to the regular CHIP rate over time.
- Extends the requirement for states to maintain for coverage for children from 2019 through 2023; after October 1, 2019, the requirement is limited to children in families with incomes at or below 300% FPL.
Simmons-Duffin, Selena. After Months in Limbo for Children's Health Insurance, Huge Relief over Deal, National Public Radio: All Things Considered. https://www.npr.org/sections/health-shots/2018/01/23/580062690/after-months-in-limbo-for-childrens-health-insurance-huge-relief-over-deal. January 28, 2018.
Shapiro, Lisa. The Children's Health Insurance Program: Key Facts About CHIP and How it Helps Kids, First Focus. https://firstfocus.org/wp-content/uploads/2017/04/CHIP-Key-Facts-082317-1.pdf. Sept. 2017.
Id.
Kaiser Family Foundation. Status of Federal Funding for CHIP and Implications for States and Families, https://www.kff.org/medicaid/fact-sheet/status-of-federal-funding-for-chip-and-implications-for-states-and-families/. January 10, 2018.
Scott, Dylan. Congress just funded CHIP for a full decade. Vox, https://www.vox.com/policy-and-politics/2018/2/7/16986440/chip-funding-10-years. Updated Feb. 9, 1028.
November 2017 - Tax Reform Insight
Both chambers of Congress are actively working on comprehensive tax reform bills. The House of Representative's bill passed on Thursday, Nov. 16, while the Senate is readying for a floor vote immediately after the Thanksgiving holiday.
While neither the Senate's nor the House's legislation will be the final bill that reaches the President's desk, there are stark differences that exist between the two. The Senate's proposed bill includes the repeal of the individual mandate, a cornerstone of the Affordable Care Act. In the provision the repeal would not expire and is estimated to raise approximately $318 billion over 10 years.
The nonpartisan Congressional Budget Office (CBO) has released an updated estimate in response to possible repeal of the individual mandate within the confines of the existing health care law. The number of uninsured will increase by 4 million in 2019 and 13 million by 2027. The CBO acknowledges the difficulty in projecting these numbers, but stated the following, "Despite the uncertainty, some effects of this policy are clear: For instance, the federal deficit would be many billions of dollars lower than under current law, and the number of uninsured people would be millions higher."
NANN is committed to advocating for affordable access to quality care for all. Under the existing health care law, removing the individual mandate at this time will have harmful effects on patient care. It is in the best interest of our patients and families for a fully vetted, scored, and debated health care legislation to be created.
The Senate is currently in recess and will reconvene on Monday, Nov. 27. Now is the time to make your voice heard – contact your Senators today!
As the tax reform bill continues to evolve, NANN will keep members abreast of new developments. If you have any questions, please contact Joe Lindahl, Sr. Operations Manager, at This email address is being protected from spambots. You need JavaScript enabled to view it..
September 2017 - Global Goal: Reducing Maternal Child Mortality
 Julie Sundermeier, DNP APRN NNP-BC
Julie Sundermeier, DNP APRN NNP-BC
Between 1990 and 2015, maternal mortality worldwide dropped by about 44%. While a significant improvement, every day approximately 830 women around the world continue to die from mostly preventable causes related to pregnancy and childbirth. During that same time period mortality rates for children under five were reduced by more than one half. Yet 16,000 children under the age of five continue to die daily. A 2015 United Nations report notes that 45% of all under-five deaths happen during the first 28 days of life, one million neonatal deaths occur on the day of birth, and close to two million children die in the first week of life.
A reintroduced piece of bipartisan legislation, the Reach Every Mother and Child Act of 2017 (S. 1730), has the goal to implement a strategic approach for providing foreign assistance in order to end preventable child and maternal deaths globally by 2030. This legislation would assist in the effort to end preventable deaths of mothers and children under five. The bill was introduced by Senators Susan Collins (R-ME), Chris Coons (D-DE), Johnny Isakson (R-GA), Jerry Moran (R-KS), Dick Durbin (D-IL), Jeanne Shaheen (D-NH), Marco Rubio (R-FL), Mike Enzi (R-WY), Chris Murphy (D-CT), and Richard Blumenthal (D-CT). This bill will soon be introduced in the House of Representatives.
The Reach Every Mother and Child Act 2017 would:
- Establish rigorous reporting requirements to improve transparency, accountability, efficiency, and oversight of maternal and child health programs
- Coordinate a U.S. government strategy to end preventable maternal, newborn and child deaths and help ensure healthy lives by 2030
- Ensure that the United States Agency for International Development (USAID) scales up the most effective programs
- Encourage the use of innovative ways to pay for these programs, including public-private partnerships
- Focus on the poorest and most vulnerable -populations, recognizing the unique needs of different countries and communities
- Improve coordination among the U.S. government agencies and relevant foreign governments and international organizations
- Accelerate partner country progress toward self-sustainability for maternal, newborn and child health
Contact your Senators to voice your support of reducing maternal child mortality at a global level.
References
UNICEF. Retrieved from http://www.childmortality.org
World Health Organization. Retrieved from http://www.who.int/mediacentre/factsheets/fs348/en/
You D., et al. (2015). Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. doi.org/10.1016/S0140-6736(15)00120-8
July 2017 - Health Care Reform: What Now?
 Elizabeth Welch-Carre, EdD MSN APRN NNP-BC
Elizabeth Welch-Carre, EdD MSN APRN NNP-BC
Last week was dramatic in the Senate as several bills that would change or repeal the Affordable Healthcare Act (AC) were introduced. Ultimately, the Senate could not pass any legislation that affects the current health care law in place.
On July 25th, by a vote of 51 to 50, the Senate passed a motion to begin debate to repeal the Affordable Care Act (ACA). All 48 Democrats and two Republican Senators opposed the motion. However, Vice-President Pence cast the tie-breaking vote allowing the debate to commence (Stark, 2017) and allowed what is called "vote-o-rama" to commence. During this time period all members of Congress were invited to propose new amendments to be voted upon before the bill is finalized.
The final bill was brought to the floor in the form of a "skinny bill" which would have
- Removed some of the ACA mandates
- Increase the number of uninsured to 43 million by 2026 (CBO, 2016)
- Increase premiums for non-group members by as much as 20% (CBO, 2016)
- Medicaid coverage for infants who need it
- No per capita cap because many infants may reach that cap early in life
- Continued coverage of essential health benefits:
- Ambulatory patient services
- Emergency Services
- Hospitalization
- Maternity and newborn care
- Mental health and substance use disorder treatment, including behavioral health
- Prescription drug coverage
- Lab services
- Preventative and wellness services and chronic disease management
- Pediatric services which include oral and vision care
- Continued coverage of pre-existing conditions because a) many infants have congenital conditions and b) many pregnant women/mothers have pre-existing conditions
The future of health care reform is unclear. The Senate GOP has stated that they wanted to change their focus to other legislation, most notably tax reform and infrastructure. However, both parties have maintained that they want to improve and stabilize the current health care market (Schroeder, 2017). President Trump is still encouraging the Republicans to find a replacement bill for the ACA. A bipartisan group of House members, called the Problem Solvers Caucus, are also gathering to discuss ways to improve the existing healthcare law.
NANN will continue to provide updates and advocate for the following:
Works Cited
Bryan, B. (2017, July 13). The Business Insider. Retrieved from Business Insider: http://www.businessinsider.com/ted-cruz-amendment-health-care-bill-preexisting-conditions-2017-7
Congressional Budget Office. (2016, December ). Congressional Budget Office. Retrieved from Congressional Budget Office: https://www.cbo.gov/budget-options/2016/52232
Congressional Budget Office. (2017, July 19). Cost estimate: H.R. 1628 Obamacare Repeal Reconciliation Act of 2017. Retrieved from https://www.cbo.gov/system/files/115th-congress-2017-2018/costestimate/52939-hr1628amendment.pdf
Krieg, G. (2017, June 26). CNN. Retrieved from CNN: http://www.cnn.com/2017/06/22/politics/comparing-obamacare-ahca-senate-health-care-bill/index.html
Ohlemacher, S., & Taylor, A. (2017, July 26). ABC News. Retrieved from ABC News: http://abcnews.go.com/Health/wireStory/senate-health-care-debate-suspenseful-raucous-48853633
Ramsey, L. (2017, July 26). Business Insider. Retrieved from Business Insider: http://www.businessinsider.com/senate-health-care-vote-repeal-without-replace-2017-7
Schroeder, R. (2017, July 30). Market Watch. Retrieved from Market Watch: http://www.marketwatch.com/story/where-health-care-reform-goes-after-failure-to-repeal-and-replace-obamacare-2017-07-28
Stark, L. (2017, July 25). Vote tally: How each senator voted on GOP health care motion. Retrieved from CNN.com: http://www.cnn.com/2017/07/25/politics/vote-tally-senate-health-care/index.html
June 2017 - the ACHA and Maternal Child Health
Julie Sundermeier, DNP, APRN, NNP-BCChair, Health Policy and Advocacy Committee
H. R. 1628, the American Health Care Act (ACHA), has been in the spotlight with the House passing the bill by a narrow margin on May 4, 2017. This legislation would repeal and replace parts of the Affordable Care Act and has raised opposition from numerous notable medical organizations such as the American Medical Association, American Academy of Pediatrics, and American Nurses Association.
Among the concerns is the anticipated exponential increase in uninsured Americans. The Congressional Budget Office (CBO), a non-partisan office that provides independent analyses of budgetary and economic issues, published a report stating that there would reduction in the Federal deficit by $119 billion over the course of 2017 to 2026, and that "the largest savings would come from reductions in outlays for Medicaid and from the replacement of the Affordable Care Act's (ACA's) subsidies for nongroup health insurance". As a result, according to CBO's findings, 14 million more people would be uninsured in 2018, 19 million more in 2020, and an estimated 23 million more in 2026 compared to current law (Congressional Budget Office, May 24, 2017).
NANN is committed to advocating for maternal child health. The ACHA legislation passed by the House would have direct impact on the heath and welfare of the population we care for. Currently there are 37 million children that benefit from Medicaid and a record 95% of children across the United States currently have health coverage (Stein, 2017). The ACHA legislation passed by the House will have deleterious effects for maternal and child healthcare, impacting NICU patients and graduates directly.
H. R. 1628 (ACHA) as written would:
- Convert federal Medicaid financing to a per capita cap beginning in FY 2020. Federal share of payments would be capped with pre-set amount per enrollee (total or by population group)
- Preterm and sick infants could potentially reach their cap with a lengthy and involved initial hospital course.
- Babies who survive a premature birth and hospitalization may have lifelong health problems such as cerebral palsy, vision and hearing loss, and intellectual disabilities.
- Children born with congenital malformations and defects may require multiple surgeries and prolonged periods of hospitalization.
- Implementing a per capita cap could be difficult administratively and maintain current inequities across states (Rudowitz, 2016).
- Add state option to elect Medicaid block grant instead of per capita cap for certain populations for a period of 10 fiscal years, beginning in FY 2020. States would have a set amount of money for Medicaid spending
- Block grants could limit funding of important programs such as funding to public schools to provide early intervention services.
- Fewer individuals would qualify for Medicaid.
- In states electing Medicaid block grant, family planning would no longer be a mandatory covered service (Henry J Kaiser Family Foundation, 2017).
- Continue the ACA requirement to cover 10 essential health benefit (EHB) categories. All women and children benefit from the inclusion of these benefits.
- Ambulatory patient services
- Emergency Services
- Hospitalization
- Maternity and newborn care
- Mental health and substance use disorder treatment, including behavioral health treatment
- Prescription drugs
- Rehabilitative and habilitative services and devices
- Lab services
- Preventive and wellness services and chronic disease management
- Pediatric services, including oral and vision care
However...starting in 2020, essential healthcare benefits, including maternity and newborn care, could be changed under state waiver authority (Kaiser, 2017). The CBO (2017) projects that "those living in states modifying the EHBs who used services or benefits no longer included in the EHBs would experience substantial increases in out-of-pocket spending on health care or would choose to forgo the services. Services or benefits likely to be excluded from the EHBs in some states include maternity care, mental health and substance abuse benefits, rehabilitative and habilitative services, and pediatric dental benefits. In particular, out-of-pocket spending on maternity care and mental health and substance abuse services could increase by thousands of dollars in a given year for the nongroup enrollees who would use those services." (CBO, March 13, 2017).
Weakening the rule of essential health care will allow insurers to charge people with pre-existing conditions higher premiums. It will also allow insurers to deny people coverage for the care and services they need. This could affect not only people in the individual market but also those who get their health insurance through employers.
Low maternal income or socioeconomic status is associated with preterm birth. If a mother cannot afford out of pocket expenses, prenatal care may be sporadic or deferred.
- Prohibit federal Medicaid payments to Planed Parenthood
- Federal law already prohibits federal dollars from being used to pay for abortions other than those to terminate pregnancies that are a result of rape, incest or a threat to the pregnant woman's life. (Ranji et al, 2017).
- Cutting off Medicaid payments to Planned Parenthood for one year would result in loss of access to services, such as contraception) in some low-income communities. A CBO (March, 2017) report stated that the policy would result in thousands of additional unintended pregnancies that would in turn be financed by Medicaid.
The Senate is currently working on drafting their version of ACHA legislation. Details of this legislation have not been released to the public so little is known about how the Senate bill will compare to the House ACHA bill. NANN's HPAC Committee will monitor this legislation closely and update the NANN community once details are forthcoming. We encourage members to contact their representatives to educate them on how the ACHA will affect women and infants.
References
Congressional Budget Office. (May 24, 2017) Cost Estimate: H. R. 1628 American Healthcare Act of 2017. Retrieved from: https://www.cbo.gov/system/files/115th-congress-2017-2018/costestimate/hr1628aspassed.pdf
Congressional Budget Office (CBO). (March 13th, 2017). American Health Care Act. Retrieved from: https://www.cbo.gov/system/files/115th-congress-2017-2018/costestimate/americanhealthcareact.pdf
Henry J. Kaiser Family Foundation. (June 26, 2017). Summary of the American Health Care Act. Retrieved from: http://files.kff.org/attachment/Proposals-to-Replace-the-Affordable-Care-Act-Summary-of-the-American-Health-Care-Act
Ranji, U., Salganicoff, A., Sobel, L, & Rosenzweig, C. (May 8, 2017). Ten Ways That the House American Health Care Act Could Affect Women. Henry J. Kaiser Family Foundation, Retrieved from: http://www.kff.org/womens-health-policy/issue-brief/ten-ways-that-the-house-american-health-care-act-could-affect-women/
May 2017 - Nurse in Washington Internship (NIWI) and NANN
Stephanie M. Blake DNP, RN, NNP-BC
Chair-Elect, Healthy Policy and Advocacy Committee
I had the pleasure of participating in the NIWI program through the NANN NIWI Scholarship Program, which is a gathering of nursing professionals covering all spectrums of healthcare, and a forum for The Nursing Community coalition. The coalition includes 63 national nursing organizations all of which are committed to improving the health and health care of our nation through collaboration by supporting the education and practice of Registered Nurses (RNs) and Advanced Practice Registered Nurses (APRNs).
The three day internship was jam packed with all the information one needed to know on the how, when, what, and why of nursing advocacy. The first two days consisted of panels including Professional Nurse Advocates, a Congressional Staff Panel, and a General Advocacy Panel. In preparation for our day on the Hill, discussions included advocacy training and tips as well as the Nursing Community coalition "Asks". Representative Gail Adcock, MSN, RN, FNP-BC, FAANP, North Carolina House of Representatives and the first APRN elected to the North Carolina legislature, was the featured speaker, who was dynamic and inspiring. Her poignant discussion of her life in politics and work experiences as a Family Nurse Practitioner that led her to where she is today was as comical as it was serious. Listening to Rep.Adcock left all attendees feeling as if it is time to get up, make our voices heard, and advocate for change.
Day three was comprised of meetings on the Hill where these three "Asks" were given to each attendee's home state House Representative as well as Senate Representative.
Ask 1: $244 million for the Title VIII Nursing Workforce Development Programs in FY 2018.
In order to ensure access to care across the nation, investments in the pipeline of RNs and APRNs must remain a top priority. While great strides have been made to meet the demand for nurses, a constant focus must be placed on education to ensure a stable workforce. This could not be truer in communities struggling to recruit and retain highly qualified providers, including those in rural and medically-underserved regions.
For over 50 years, the Nursing Workforce Development Programs (Title VIII of the Public Health Service Act [42 U.S.C. 296 et seq.]) have helped to meet the nation's demand for nurses. More than ever, safeguarding dollars to promote America's health through nursing care is critical. These dollars translate to on-the-ground care being delivered in all corners of the country. For example, in Academic Year 2014-
2015, the Title VIII Advanced Nursing Education Grants supported 9,024 graduate nursing students and partnered with over 4,200 clinical training sites. Of these, 45% were located in underserved areas and 46% provided primary care.
Update: Since our visit to the Hill, President Trump released his FY 2018 Budget Proposal which recommends to Congress steep cuts to HHS programs. The proposal suggests the Title VIII Nursing Workforce Development programs be decimated by 64% taking the funding level from $229.472 million in FY 2017 down to $82.977 million. To put this in context, this is slightly more than the programs received back in FY 2001. Essentially, what the budget recommends is to only fund the NURSE Corps (Loan Repayment and Scholarship program-*note 0.19% decrease from the Omnibus, not the CR as reported in the justification) and eliminates the funding for the following Title VIII programs:
- Advanced Nursing Education Grants (ANE), ANE Traineeships, and Nurse Anesthetist Traineeships
- Nurse Education, Practice, Quality, and Retention Program
- Nurse Faculty Loan Program
- Nursing Workforce Diversity Grant
- Comprehensive Geriatric Education Grants
Ask 2: $160 million for the National Institute of Nursing Research (NINR) in FY 2018
As one of the 27 Institutes and Centers at the National Institutes of Health (NIH), NINR funds research that establishes the scientific basis for quality patient care. Nurse scientists supported by NINR are advancing discoveries in genetic research, leading team science, and promoting precision health initiatives. In addition, nurse scientists lead complex studies focused on health promotion and disease prevention. The Ad Hoc Group for Medical Research is requesting at least $2 billion above the FY 2017 funding level for the National Institutes of Health, in addition to funds included in the 21st Century Cures Act. Included in this amount is $160 million for the National Institute of Nursing Research.
Update: As it relates to the NINR, President Trump's FY 2018 budget proposes taking the funding levels back to approximately what NINR received 16 years ago. The President recommends a 24% reduction to NINR— taking the funding from $150.273 million in FY 2017 down to $113.668 million. For all of NIH, the recommended cut is approximately 21% taking the funding from $32.084 billion to $26.9 billion. (Please note, the President's Budget compares the CR levels and not the final FY 2017 Omnibus).
Ask 3: Join the Nursing Caucus
The bipartisan House and Senate Nursing Caucuses educate legislators on issues impacting the profession and how nurses are transforming America's health.
NIWI is not only for the novice nurse wanting to learn about advocacy, but for the experienced advocacy nurse as well, offering continued opportunities to advocate for the nursing community that we are all a part of. NANN will have additional information on the 2018 NIWI Scholarship program available after the Annual Conference in October.
References
- http://www.nursing-alliance.org/About-Us
- Health Resources and Services Administration. (2016) Justification of estimates for appropriations committees. Retrieved from: https://www.hrsa.gov/about/budget/budgetjustification2017.pdf
For more information about the Nursing Community requests, contact Convener of the Nursing Community, Dr. Suzanne Miyamoto, at This email address is being protected from spambots. You need JavaScript enabled to view it.
April 2017 - 3 Quick and Simple Advocacy Tools
Keeping track of legislation can be intimidating. Bills are constantly changing, elected official's priorities are ever-shifting, and schedules are rarely kept. Throw in the multiple layers of federal, state, and municipalities - knowing what is going on in the world of public policy and advocacy can be near impossible. As a starting point, The Health Policy and Advocacy Committee (HPAC) has three simple (and free!) tools to help you stay current on legislation.
 GovTrack
GovTrack
By Lizz Welch-Carre, MS NNP-BC
Govtrack is a non-partisan one-stop shop to learn more about legislative bills. The website allows you to set up alerts so that you can receive updates about bills that are important to you (such as nursing or healthcare). You can also receive a customized email each week with all of the bills and resolutions that have been submitted over the last. If you provide your address, the website will give you the names of your Representative and Senators – it even provides information about their voting record. GovTrack also has links to all of the legislative committees for Congress. It lists the names of the chair and all of the members of the committee and tracks committee activity or any of the subcommittees.
Follow @govtrack or Facebook help you stayed informed via social media.
 OpenStates.org
OpenStates.org
By Tommie Farrell, BSN RNC
If you're interested in more local and state specific legislation, OpenStates.org may be the website for you. Open States is an open source website run by volunteers that allows you to connect to your legislators in all 50 states, Washington D.C., and Puerto Rico. The website also allows you to track active or pending state legislation, the progress of bills, and how your legislator is voting. Data on the website is extensive and reliable, all of which is shareable via Twitter and Facebook.
There is a link to a user friendly tutorial on how to use this site and Open States is on Twitter at @openstates.
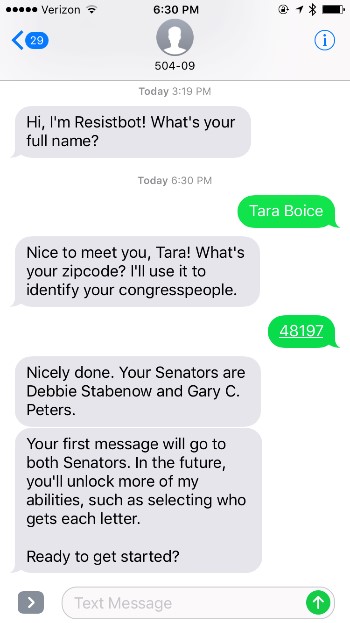 Resist Bot
Resist Bot
By Tara Boice
Resistbot is a new, free service that turns text messages into faxes and sends them to your elected officials. Unlike pre-written form letters, which are often ignored by Congress, Resistbot doesn't tell you what to say. Your own personal message as a constituent and nursing professional can be more effective in reaching your representative. By texting "resist" to 50409 and answering a few simple questions, you will be able to generate personalized fax messages to your senators. Over time, Resistbot allows users access to more features such as the ability to contact your U.S. Representative.
No worries- messages don't have to be polished essays. A couple of sentences from a real voter can be very impactful. Just text "resist" to 50409 and in five minutes you can send two letters to your Senator. It's really that easy! Follow Resistbot @botresist on Twitter
March 2017 - Withdrawl of the American Health Care Act
In the February issue of From the Hill to the NICU, we discussed the Republican administration's plan to "repeal and transition" the Affordable Care Act (also known as the ACA or Obamacare) and saw the transition plan in March. The GOP's bill, the American Health Care Act (also known as the AHCA or Trumpcare), was a moving target up until the day of the vote as House Speaker Paul Ryan tried to amend portions of the bill that would appease the Freedom Caucus, the most conservative wing of the Republican Party. The final version of the AHCA that was debated included the elimination of essential health care benefits—including prenatal and maternal health care.
NANN issued a call to action opposing the AHCA as the House of Representatives planned to vote on the bill on Friday, March 24th. After four hours of debate, the AHCA was withdrawn after party leadership realized it did not have enough votes to pass.
The withdrawal of the AHCA leaves the ACA intact as the Republicans turn their attention towards tax reform.
What does this mean for us?
The ACA, signed into law in 2010 and enacted in 2014, still stands as federal law. States such as Kansas and North Carolina will now look at Medicaid expansion, knowing the ACA will remain the health care law for the foreseeable future. There will be two governorships up in 2017 (VA and NJ) and 39 up in 2018 (36 states, three territories). Health care will be a hot topic for all elections.
The Health Policy and Advocacy Committee is committed to working with other nursing organizations to monitor the ongoing communications on Capitol Hill. As additional information becomes available on health care legislation and other issues relevant to neonatal care, NANN will keep its members abreast with pertinent and timely updates.
February 2017 - Patient Protection Affordable Care Act
Elizabeth Welch-Carre, MS NNP-BC
The Patient Protection Affordable Care Act, also known as the ACA or Obamacare, will be repealed by the Republican Party who controls the legislative and now executive branch of the federal government. The repeal will be done through budget reconciliation, which will eliminate the employer and participant penalties associated with the act, effectively making the law non-existent. This process is also how the ACA was originally passed.
Repeal and Transition
The GOP changed their initial tagline of "repeal and replace" to "repeal and transition," to accurately communicate the timeline needed to alter the existing law. As of this writing, no ACA replacement plan has been introduced into Congress, but there have been several possible plans discussed which include the following:
- Medicaid may be changed to block grants for states which would provide enrollees with a set amount of money for coverage
- Provide subsidies for premium coverage, instead provide tax breaks
- Likely will repeal the individual mandate for coverage
- States will be allowed to keep ACA if desired
- Cover pre-existing conditions but may be in high-risk pool
- Continue with coverage for offspring up to age of 26
What does this mean for us?
NANN is committed to working with other nursing organizations to monitor the ongoing communications on the hill. As it pertains to neonatal nurses and the specific population we provide care for, the following topics are on the HPAC's radar:
- Pregnancy and newborn care
- Breastfeeding benefits
- Covers the cost of breast pumps
- Substance use disorder treatment
- Mental Health Services
- Treatment for behavioral health diagnosis
- Substance use disorder treatment
- Pre-existing condition coverage
- Continuous health insurance coverage provided for pregnant women
- Continuous coverage for other pre-existing conditions that may impact pregnancy
- Preventative care woman
- STD testing and treatment
- Tobacco screening and treatment
- Breast cancer screening
- Preventative care kids
- Immunizations
- Developmental screening 0 to three years
- Well-baby appointments
As additional information becomes available on this ongoing issue, NANN will keep our members abreast of pertinent and timely information.
If you have any questions regarding the Patient Protection Affordable Care Act or the Health Policy and Advocacy Committee, please contact Joe Lindahl, NANN Senior Operations Manager, at This email address is being protected from spambots. You need JavaScript enabled to view it..